Lyme disease toolkit
Lyme disease, or Lyme borreliosis, is named after Old Lyme, a town in Connecticut, USA. In the 1970s, lots of children developed symptoms similar to juvenile arthritis in the town. However, its dermatological and neurological manifestations have been recognised in Europe since the late 1800s. Bannwarth’s syndrome, lymphocytic meningo-radiculitis, was described in 1941. A variant of Borrelia burgdorferi DNA has since been identified in the ice-age mummy, Ötzi.
There are many species of Borrelia worldwide, and those which cause Lyme disease are referred to as Borrelia burgdorferi sensu lato (Bbsl). In the UK, there are three main genospecies known to cause Lyme disease and symptoms may vary depending on the species:
- Borrelia garinii (Bg) is associated with neurological conditions
- Borrelia afzelii (Ba) is associated with skin and atypical neurological presentations
- Borrelia burgdorferi sensu stricto (Bbss), may cause Lyme arthritis, especially of large joints such as the knee
Borrelia burgdorferi sensu stricto is the main cause of Lyme disease in the USA. The American strains of Bbsl are thought to cause a more severe inflammatory reaction, and have been associated with fatal Lyme carditis.
1. Epidemiology
Lyme disease occurs throughout most of the world and is the most common tick-borne disease in the Northern hemisphere. The incidence has been increasing, possibly due to climate change, changes in land management and biodiversity, as well as increased awareness. In the UK official figures only include laboratory-confirmed cases, and do not include those diagnosed clinically. Some cases may also be misdiagnosed or go unreported, so the official figures are known to underestimate the true scale of the problem.
- Public Health England - Lyme disease epidemiology and surveillance
- Zoonotic disease in Scotland, 2019
- Health Protection Scotland - Lyme Disease, Annual Totals
A proportion of cases are contracted after foreign travel. The recorded incidence of Lyme disease is higher in continental Europe compared to the UK, especially eastern European countries. The North-Eastern USA and West Coast are also highly endemic areas.
2. Ticks and Tick Bites
A. Ticks
- Ticks are small blood-sucking arthropods that are found across the UK.
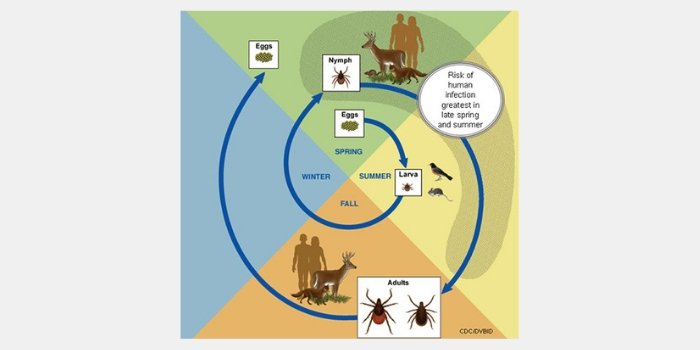
- Ticks hatch and moult through three life stages: larva, nymph and adult.
- Ixodes ricinus or sheep tick
- Ixodes hexagonus or hedgehog tick, which may inhabit urban areas
- Ixodes canisuga: the fox tick, also known as the dog tick
- N.B. Ixodes scapularis is the deer tick, a native American species, not found in the UK
- Ticks need humidity and shade to survive. They are found in woods, fields and moorland but may survive in urban parks and gardens if conditions are suitable, including areas of Central London.
B. Tick exposure outside the UK
European tick maps
USA tick maps
Advice on avoidance and prevention of tick bites includes:
- Avoid brushing against vegetation
- Wear long trousers and tuck them into socks
- Wear light coloured clothing so that ticks are more easily noticed
- Carry out tick checks - especially on children and domestic animals
- Prompt correct tick removal is key to primary prevention of Lyme disease.
- Insect repellents containing DEET and picardine are effective against ticks.
- Pet owners are one and a half times more likely to be bitten by a tick than non-pet owners. (Animals may carry ticks into the home.)
Public Health England - Lyme disease prevention
Public Health England tick awareness leaflet
Tick bite prevention and management
C. Tick bite management
- Only one in three people are thought to notice a tick bite
- Nymphs, the stage most likely to bite humans, may be as small as a poppy seed so may not be noticed.,/li>
- Ticks feed and may remain firmly attached for up to five days in order to take a blood meal. Tick saliva contains anti-inflammatory and anti-clotting agents, so the bite may not be itchy or painful.
- Adults tend to be bitten on the lower body such as behind the knee, the groin or the navel, whereas children may be bitten on the upper body, especially around the hairline.
- The statistical risk of a person developing Lyme disease from a tick bite in the UK is thought to be low. However, it only takes one bite from an infected tick for infection to be transmitted, especially if the tick remains attached for long enough to become engorged. There is no proven minimum time of attachment required for transmission of infection.
- Ticks should be removed promptly and carefully using fine-tipped tweezers or a tick removal tool. Do not use oil or nail varnish. Avoid squashing the tick.
- A person who has been bitten by a tick should remain vigilant for signs of skin rashes, flu-like symptoms or other unusual symptoms for at least 30 days following the bite and seek medical attention if necessary.
Images of attached ticks

3. Clinical Features
Clinical signs and symptoms of Lyme disease may be non-specific and atypical. The clinician should enquire about recent or past tick exposure, tick bites or possible erythema migrans rash. A high index of clinical suspicion may be needed to make the diagnosis.
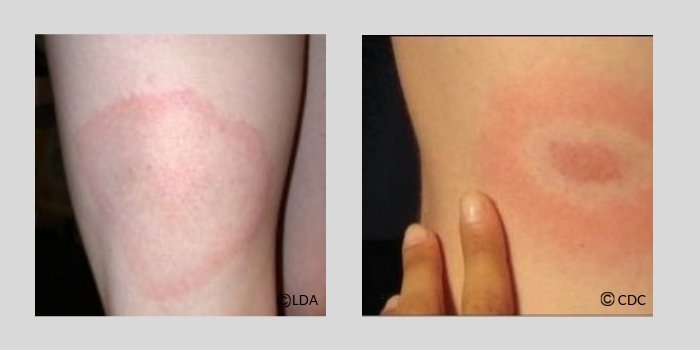
Erythema migrans
An EM (bull’s eye) rash is diagnostic but may not be present in around 30% of UK Lyme patients. It usually develops within three to 30 days of a tick bite, but may take longer. It may appear as an area of uniform redness rather than a ‘bull’s eye’ and is typically painless and not itchy. It will usually present at the site of the bite, however in early or late disseminated disease there may be multiple, sometimes transient, erythema migrans rashes on other areas of the body.
An EM rash may resolve spontaneously without antibiotic treatment. However this does not indicate that the infection itself has resolved. If left untreated the disease may disseminate around the body.
A small localised area of redness may occur in response to a tick bite but this usually resolves in -5 days and is probably not an indication of Lyme disease.
Systemic symptoms
The infection may disseminate around the body at an early stage of the disease. It may result in a multi-systemic illness involving the nervous system, joints, skin, heart and eyes. Lyme disease is known to adversely affect the immune system which may result in a relapsing-remitting clinical picture, often characterised by pain and fatigue.
Symptoms may resemble many other conditions such as facial palsy, ME/CFS, fibromyalgia, polymyalgia rheumatica, MS, motor neurone disease, carditis, meningitis, encephalitis, auto-immune conditions or neuropsychiatric problems.
In the UK and Europe, disseminated Lyme disease is more likely to affect the nervous system, (peripheral, central and autonomic), with the potential to cause a wide range of diverse neurological symptoms. Lyme arthritis is more typically seen in North America.
Early diagnosis and adequate treatment provide the best chance of cure. Late diagnosis and inadequate treatment may result in continuing health problems and on rare occasions life-threatening consequences.
4. Scientific uncertainties and conflicting opinions
There is ongoing medical and scientific uncertainty and conflicting opinion in relation to many aspects of diagnosis and treatment of Lyme disease. There is a recognised need for further research in order to address core uncertainties and improve patient outcomes.