Deafness and hearing loss toolkit
Information for NHS Managers and Carers
NHS England Commissioning Services for People with Hearing Loss: A framework for clinical commissioning groups or networks
The commissioning framework is designed to support the commissioning of non-specialist services for people with hearing loss, across a spectrum of providers to improve quality, access and consistency; therefore, benefitting the people who need to use hearing loss services. The framework provides clear guidance on what good commissioning for hearing loss services looks like. Responsibility is placed firmly at a local level to meet the needs of varying populations. The framework aims to support the delivery of more integrated hearing services, closer to home delivering better outcomes and value for people with hearing loss.
The document sets out clear information and guidance on the following topics
- Why we need a Commissioning Framework for Hearing Services
- What Matters to People with Hearing Loss
- Principles for Commissioning Hearing Services
- Planning Hearing Services
- Securing Hearing Services that Deliver Improved Outcomes and Value
- Monitoring for Quality Improvement
- Commissioning Models – Case Studies
- Moving Forward
NHS England has published the full commissioning framework online.
Key points and important messages for GPs from the hearing loss commissioning framework
Local commissioning services should be aware of the impact of hearing loss and its association with physical health, mental health, dementia, falls and other health issues. These remain as policy priorities for the Government and the NHS along with addressing the continuing variation in access and quality of hearing loss services.
The Adult Hearing Service must be seen as part of wider integrated adult health and social care hearing services that work in partnership with GPs, primary health care teams, ENT departments, audio-vestibular medicine (AVM) audiology departments, local authorities (including social care and educational services), the voluntary and community sector and independent providers.
The Hearing Loss and Deafness Alliance has developed principles to help inform the commissioning of services to protect and deliver complete hearing wellbeing for individuals and populations. The main themes for the principles are focused on ensuring that commissioning:
- Promotes excellence in outcomes for patients;
- Is clinically and service user led;
- Supports evidence-based practice; and
- Facilitates choice and flexibility in provision of services
It is very important that a clear local pathway is developed and understood to deal with ear wax before audiological assessment is undertaken; visits to audiology, prior to wax being checked and removed, are a significant source of inappropriate referrals.
The NICE guidance 2018 (NG98) and NICE Quality standard (2019) are clear that such a common condition should be treated by trained staff in primary care. Commissioners should ensure that they commission services with the appropriate equipment, capacity and expertise to carry out earwax removal for adults in primary or community care. For adults with earwax that is affecting hearing, causing other symptoms, stopping appropriate ear examination or blocking an impression of the ear canal to be taken, earwax removal closer to home should be provided. Ideally this would be in primary care or community-based ear care services, preventing the inappropriate use of specialist services.
Community-based aftercare support significantly reduces the burden on audiology departments, contributing to significant cost savings for the system. It also reduces unnecessary GP appointments and other health and social care interventions resulting from basic needs not being met.
Hearing aids, information, tinnitus retraining therapy, cognitive behavioural therapy and other specialist support are among the services that can provide help for people with tinnitus, which are usually accessed in audiology departments after referral from the GP.
Providers should provide domiciliary care to individuals who require it – the Provider should provide all parts of the service at the patient’s domicile (including residential or nursing homes) where this is requested in writing by a GP.
Commissioning should be outcome driven. Figure 1. Sets out the key outcomes for hearing services.

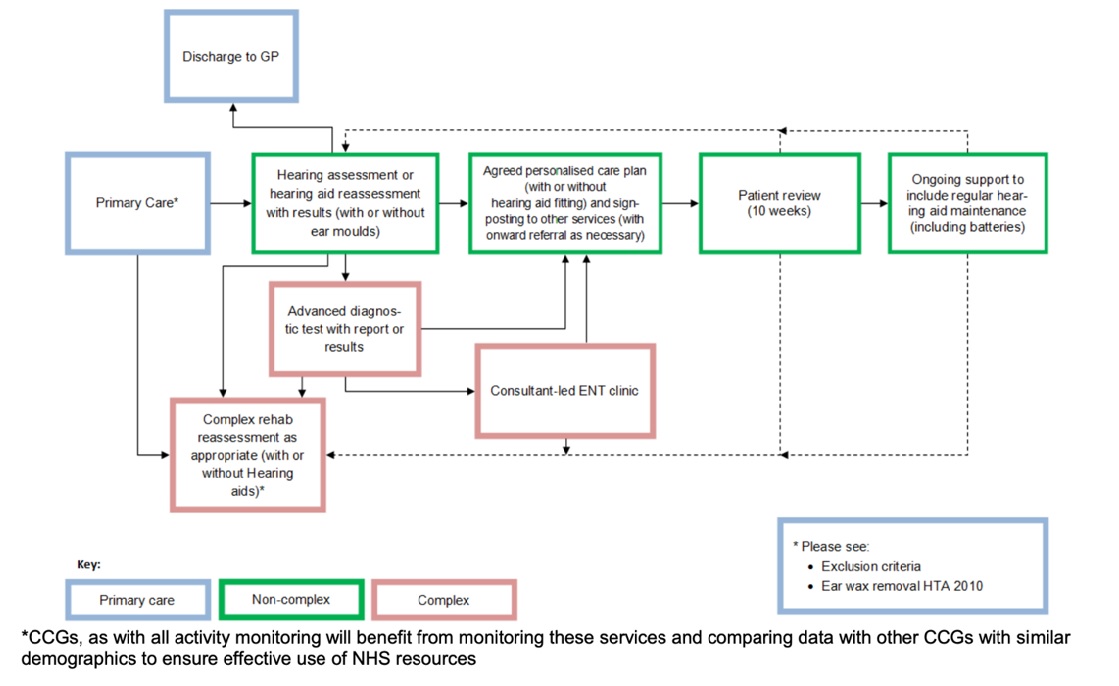
Example hearing services pathway can be seen on figure 2.
Key Performance indicators for non-specialist hearing services include:
Referral to Assessment - Time Assessments to be completed within 16 working days following receipt of referral, unless patient requests otherwise.
Assessment to Fitting - Time Hearing aids to be fitted within 20 working days following assessment, unless patient requests otherwise