Syncope toolkit
Syncope is very common and will affect 42% of people during their lifetime
Postural tachycardia syndrome (PoTS)
Postural Tachycardia Syndrome (PoTS) was named and defined in 1993. Affected patients experience a persistent tachycardia on standing, associated with debilitating symptoms of orthostatic intolerance (most commonly light headedness, palpitations and fatigue). In the UK, up to 60% of patients describe syncope.
It is a heterogenous group of disorders that usually afflicts younger women. The pathophysiology of PoTS is not well understood; it seems likely that there are multiple aetiologies.
For more information about diagnosis and management of PoTS in primary care, see:
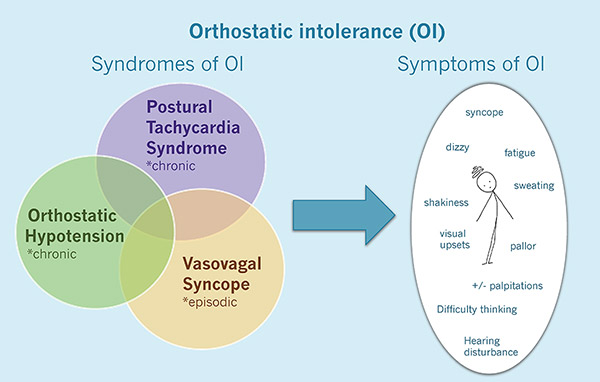
Overlap between vasovagal syncope, orthostatic hypotension and PoTS
Further reading
- PoTS UK leaflets and resources
- A brief overview of PoTS for GPs – ‘PoTS on a page’ (PDF)
- Canadian Cardiovascular Society position statement on Postural orthostatic Tachycardia Syndrome (PoTS) and related disorders of chronic orthostatic intolerance
- An open access journal supplement explaining PoTS and its management in detail
- Videos of educational lectures and PowerPoint slides on PoTS for healthcare professionals.
Postural Tachycardia Syndrome (PoTS) case history
History
A 29 year old woman consults with you due to daily symptoms over the previous 12 months of pre syncope, fatigue and palpitations following a viral illness. She recalls 3 definite syncopal episodes and had attributed these to being dehydrated and therefore had not sought medical attention previously. These syncopal episodes appeared to occur after she had been standing for long periods of time as a retail worker. She has no significant past medical history and is not taking any medication.
Examination
Physical examination is normal and postural blood pressures showed no significant drop, but her heart rate increases from 82 bpm whilst sitting to 124 bpm when standing with associated light-headedness and fast palpitations.
Which investigations should be performed in primary care?
An ECG should be performed, and this is normal. She should also have U+E, TFTs, and an FBC. Consider a glandular fever screening test.
What would you do next?
The increase in her heart rate on standing raises the possibility of postural tachycardia syndrome (PoTS) and she should be referred to a local cardiologist with an interest in PoTS for further assessment.
Outcome
The cardiologist organises a 24-hour Holter monitor which shows sinus rhythm ranging from 62 bpm to 168 bpm; the recurrent tachycardias relate to periods of activity during the day.
She undergoes a tilt table test which reveals a persistent increase in her heart rate from 75 bpm to 125 bpm on passive tilting. Nitroglycerin is administered which shows a further rise in heart rate followed by a fall in blood pressure and an asystolic pause associated with syncope. She is diagnosed with postural tachycardia syndrome and vasovagal syncope. She starts treatment with advice on fluid and salt intake and gentle supine exercise. Later fludrocortisone is added with good symptom control when she was followed up.
Learning points
- PoTS is characterised by chronic symptoms including light headedness, weakness, palpitations and fatigue especially when upright
- There is a persistent increase in heart rate of over 30 bpm from supine to the upright position without a reciprocal fall in blood pressure.
- Some patients have episodes of vasovagal syncope, but its incidence is similar to that of the general population.
- Stand test can diagnose PoTS and a tilt table test is useful in patients with an unclear cause for their symptoms.
- Secondary care clinicians with an interest in PoTS may be found in cardiology, neurology, medicine for the elderly and paediatric departments. In some areas of the UK there are no specialists available and out of area referrals may be necessary, especially for complex patients.