Royal College of General Practitioners - Online Learning Environment
Site blog
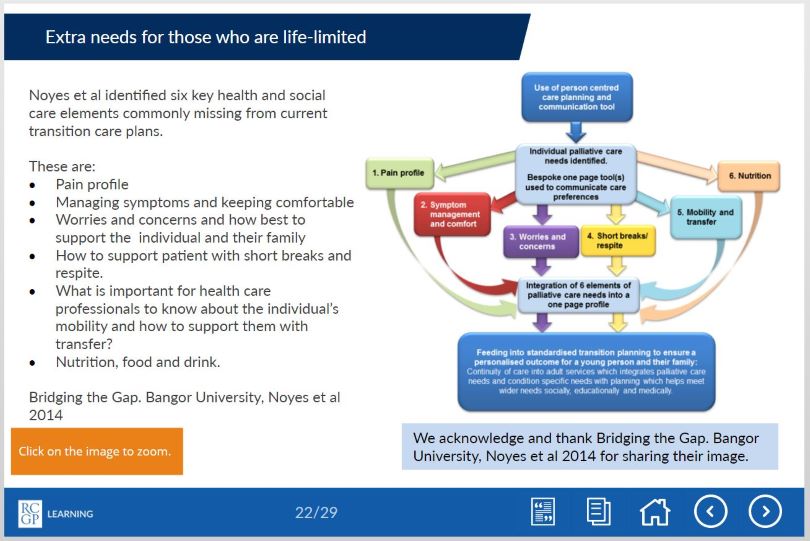
Children with life-limiting conditions face significant challenges when they transition from paediatric to adult care. The transition involves many changes: the young person will transfer to adult specialities, to adult social care, and will experience changes in educational provision and legal changes involving parental responsibility for medical decision making.
The transition has been described as a ‘cliff-edge’ event, during which children and their families face significant stress, challenges, and unmet needs. When general practice is already aware of such a patient within their practice, a good service is already provided in many cases, but often young people with these conditions are not always visible, as the majority of their care is provided by paediatrics. Many of these young patients who thus far have had long term continuity of care from their paediatricians feel nervous or have little confidence in general practice and their ability to meet their complex needs. In some cases this can lead to ‘fire-fighting’, where general practice has to respond to crisis calls from young people (or their carers) with whom they may have had limited contact.
Recently, a small team at the RCGP – together with their colleagues from ‘Together for Short Lives’, produced an eLearning course on how the whole primary care team can contribute towards a good health transition from paediatric to adult care. These modules are for all primary care clinicians who want to provide excellent care for a young person with a chronic and/or life-limiting condition who is transitioning from paediatric to adult care. The modules are based on the insights generated by a pilot project which involved a steering group inclusive of general practice, palliative care, paediatricians, academics, and ‘Together for Short Lives’. Written by Dr Mike Miller, a paediatric palliative consultant with first hand experience of the pitfalls during transition and Dr Peter Lindsay, a GP with a special interest in paediatrics, the course combines the latest academic insights on health transition and the experiences of the authors and the steering group team.
During the pilot project, we recognised that there is overlap between young people with chronic and/or life-limiting conditions and young people with learning disabilities, and although the groups are distinct, there are similarities in their transition process. In many areas, local transition services for young people with complex needs are evolving rapidly: Leeds have developed an evolving transition network, and so far involves ongoing collaborations between education, the local children's hospice, social care, mental health services and learning disability leads.
As part of the pilot project, we performed initial searches within our practices for patients within these categories, and are now trying to develop processes to support transition. The pilot project highlighted the positive impact we can have in supporting the young person and family at a challenging and stressful time, and how we can improve health and social outcomes. As well as the routine care offered, general practice is uniquely placed to offer continuity of care through the transition period, early preparation for the transition to adult service, social prescribing and the help of the whole primary care team. Primary care is also perfectly placed to address health needs that often go under-recognised in this group, such as sexual health and contraception. If we can develop mechanisms to reliably identify these patients, then young people with chronic and/or limiting conditions will benefit from all that primary care can offer.
The eLearning modules firstly outline the challenges facing young people and their families during the transition period, from the perspective of a paediatric palliative care consultant who has devoted much of his career to improving the experience of young people and their families at transition. Secondly, poorly understood areas are tackled, such as the legal framework underpinning mental capacity at transition, and the practical implications of this for the young person and family. The second module presents practical approaches and best practice to support this area in a GP setting, in the current challenging and busy context of general practice. Please see below for some tasters from the eLearning modules.
Please also see the Developing Positive Transitions for Primary Care resources section, which signposts to further key information.
If you would like to learn more please see our eLearning modules and further learning resources:
'Better transitions: improving young people’s transfer from paediatric to adult services' eLearning course: https://elearning.rcgp.org.uk/bettertransitions
'Developing Positive Transitions for Primary Care' resources page: https://elearning.rcgp.org.uk/course/info.php?id=329
No-one expects their child to die before them – it isn’t the natural order of things.
From miscarriages to stillbirths and from perinatal deaths to deaths in childhood, the death of a child is a unique type of loss.
Pregnancy loss is the most common form of child loss. It is currently estimated that one in four pregnancies ends in miscarriage1 so it is something many parents will experience. Even though they may have never been able to get to know their child, they will still feel a huge loss. They grieve the potential to get to know that child and the life they would have had. Many parents will also feel a sense of guilt following a miscarriage so it is important to look out for any hint of this and to reassure the parent that this was not their fault.
When a parent loses a child of any age, in that split second, their world is changed forever. They lose not only their child, but also many of the social networks linked to their child. They lose the potential to see that child grow up and if the child was their only child, their identity as a parent and the chance to become a grandparent. They lose not only the present but also the future. The loss of a child for this reason is very different to other types of grief.
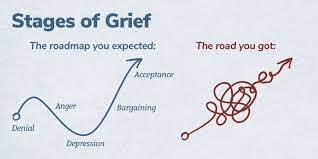 Traditionally, grief has been described in a series of stages: Denial, anger, bargaining, depression and acceptance. Current thinking has now moved towards the ‘grieving process’ as a more accurate model. Whilst grieving, it is possible to move forwards and backwards between the phases over time. Some individuals skip phases and others may spend a long time at one particular stage. Certain anniversaries or triggers may cause the grieving person to move between phases fluidly.
Traditionally, grief has been described in a series of stages: Denial, anger, bargaining, depression and acceptance. Current thinking has now moved towards the ‘grieving process’ as a more accurate model. Whilst grieving, it is possible to move forwards and backwards between the phases over time. Some individuals skip phases and others may spend a long time at one particular stage. Certain anniversaries or triggers may cause the grieving person to move between phases fluidly.
In 2007, Harper et al showed that in the 15 years after losing a child or having a stillbirth, bereaved mothers were 2-4 times more likely to die than non-bereaved mothers and that the excess risk persists for 35 years after the bereavement, though the magnitude of the risk drops with time. The increased risk persists for three years for fathers, though clearly they have an increased risk of being widowed for much longer. The reasons for this phenomenon are not clear, but could involve immunosuppression due to severe stress, maladaptive coping strategies such as alcohol misuse, pre-existing poor health which may have contributed to the child bereavement, mental ill-health following bereavement, or bereaved parents presenting later with their own physical health problems. Further research into this area would be useful. The relevance to general practice is probably that we should be aware of this risk and make particular use of the GP ‘spidey sense’ when dealing with this group of patients. Never ignore your gut feeling as a GP – it has been shown to be reliable3.
I am writing this blog from personal experience, after losing my four-year-old daughter Grace to cancer in 2014. My personal experiences have helped me to support many other families in similar situations and in 2018 I wrote an eLearning course for the RCGP, designed to provide GPs with the tools to support patients who have experienced a loss during pregnancy, or the death of an infant or child. Each family needs something different, but the overwhelming message is that having someone simply able to be there for them as a point of contact, it can make a big difference.
When a family loses a child, it also has a significant impact on their siblings. Life for their surviving siblings never returns to normal so it is important to remember that their bereavement will affect many aspects of their life and behaviour.
 “I feel like there is a piece of me missing. My friends get to play with their brothers and sisters. All I can do is look at a photo or visit his grave. It just isn’t fair. I feel on my own, and my friends don’t understand.” A bereaved sibling, aged 8.
“I feel like there is a piece of me missing. My friends get to play with their brothers and sisters. All I can do is look at a photo or visit his grave. It just isn’t fair. I feel on my own, and my friends don’t understand.” A bereaved sibling, aged 8.
Often, a few simple measures taken by a practice can make a sizable difference to help families realise that they are not alone. When the practice has been informed of a child death, it is important to contact the family, by phone if possible. This need only be brief, but families do appreciate this and remember this contact down the line.
Families should be provided with a named GP, and alerts placed on the notes of both parents and all siblings so practice staff and professionals can be aware of the history without the family needing to repeat themselves each time.
If possible, enable bereaved parents and siblings to make appointments at minimal notice for a limited time. The death of a child can plunge a family into chaos meaning things are easily forgotten or they may need to be seen quickly to help with acute emotional situations.
Ensure that all professionals are notified. Check that electronic alerts inviting the deceased child for immunisations, reviews or other routine care have been turned off. It is also useful to familiarise yourself with the services and support that are available in your local area to signpost families to as required.
General Practice is extremely busy at the moment, but these simple measures are relatively time efficient and can make a real difference to these families.
References
1 Wilcox AJ, Weinberg CR, O'Connor JF, et al. Incidence of early loss of pregnancy. N Engl J Med, 1988; 319(4): 189-94.
2 Harper M, O'Connor RC, O'Carroll RE. Increased mortality in parents bereaved in the first year of their child's life. BMJ Support Palliat Care, 2011; 1(3): 306-9.
3 Friedemann Smith C, Drew S, Ziebland S et al. Understanding the role of GPs’ gut feelings in diagnosing cancer in primary care: a systematic review and meta-analysis of existing evidence. British Journal of General Practice 2020; 70 (698): e612-e621.
'Stages of Grief' image used with permission from WPSU's Speaking Grief project.
An NIHR GM PSTRC (NIHR Greater Manchester Patient Safety Translational Research Centre) funded free e-learning course which has been accessed by 7000 prescribers since 2014 has undergone an evaluation and been re-launched with the addition of new content.
Dr Richard Knox from the University of Nottingham is one of the researchers who has worked on the e-learning course, Prescribing in General Practice. He talks about the impact of the course and the new updates here:
Prescribing in General Practice is an e-learning course, hosted on the Royal College of General Practitioners’ (RCGP’s) e-learning platform. It’s a case-based approach designed by prescribers so there’s a focus on real life examples. It was launched in 2014 and has recently undergone revisions from people who use it to ensure all the real-life examples that are used meet current guidelines. The course was also evaluated by researchers at the GM PSTRC in a new paper, which has been published in the journal Education for Primary Care.
To help assess the course’s success, in the paper, researchers used the results of a questionnaire completed by those who finished the e-learning modules. According to this the course had a positive impact on knowledge, skills and attitudes. More than 98% of 750 survey responders said the course had been a useful part of their continuing professional development.
Those who responded also wrote additional feedback and some examples are below:
“This module comprehensively covered contemporary prescribing issues particularly with respect to safety. It was grounded in everyday practice and informed by real life examples of prescribing errors and how they may occur and how to mitigate against them at an individual and at a systems level.”
“Usefully it was from the RCGP so the majority of medicines and cases presented were similar to what I would encounter on a daily basis in work. I feel from completing this module my safety and efficiency in prescribing will improve.”
“This course is going to change/improve many aspects of my prescribing practice. I would definitely spend more time on writing clear instructions for patient.”
The course was initially developed to facilitate safer prescribing among GPs. However, funding from the GM PSTRC has enabled the course to be free-to-use for all prescribers, regardless of professional background. This has increased the impact of the course which improves the safety of prescribing more widely.
The original idea for the e-learning materials came as a direct result of findings from the General Medical Council’s PRACtICe study. This was a large study of prescribing errors in UK general practice, which revealed that about one in twenty prescriptions from primary care contains an error. The PRACtICe study included a root cause analysis that helped establish a set of recommended strategies that may improve prescribing. The need to invest further in education and training was identified by all GPs, whatever their stage or experience of prescribing. A series of focus groups made up of GP trainers, GPs in training, pharmacists and members of the public also confirmed support for further training to be made available. The value of e-learning was championed – with stakeholders requesting a strong case-based approach to help inform real-world practice.
The e-learning includes five distinct lessons, each taking about thirty minutes to complete:
- Lesson one – Appropriate drug selection
- Lesson two – Avoiding prescribing errors
- Lesson three – Choosing the right drug
- Lesson four – Right dose instructions
- Lesson five – Effective medication reviews
Due to the updates the course now includes specific sections on topics such as prescribing multiple medications for the same person at the same time (polypharmacy) and the use of the Seven Step medication review process.
Please note, this course is now RCGP Members' benefit. Non-members have an option to purchase the course. You can access the Prescribing in General Practice course here.
“Medicine is an art whose magic and creative ability have long been recognised as residing in the interpersonal aspects of the patient-physician relationship1”.
Art is part of medical training from early on - lectures in medical school use images, cartoons, animations, and demonstration models. In our hospital jobs we all used drawings, lung fields with crosses, or a hexagon abdomen with a large liver on it were all used in the days of paper notes. However when asked to draw, medical students often recoil and claim that they are ‘not creative’ and cannot draw2.
We are trained in communication skills to gather information in order to facilitate accurate diagnosis, counsel and give therapeutic instructions whilst establishing caring relationships with patients3. Patients gather information from many different visual sources in the GP surgery, so using drawings is a natural next step, yet one that is rarely discussed.
We already use visual imagery in the consultation - as GPs we might point to anatomical posters in our rooms, use drawings for minor surgery consent, or the “clock test” in dementia screening. Encouraging people to see drawing as a form of learning can help them to present information more efficiently within the consultation4.
We also all use metaphor and analogy frequently - as Anatole Broyard describes, metaphors may be as necessary to illness as they are to literature and are a relief from medical terminology5. Metaphors bridge the communication gap between healthcare professionals and patients, examples including the following:
“My tongue feels weird, like licking a battery.” (Oral thrush)
“Doctor, you know when you put your hand in a bag of rice – that nice sort of tingly feeling – I get that in my head in a sort of shock.” (SSRI discontinuation syndrome)
 Clinicians can use visual metaphors; drawing a plug to describe the wrist retinaculum (Image 1) can increase understanding of the pathophysiology of carpal tunnel symptoms and be a simple start from which patients can improve their understanding.
Clinicians can use visual metaphors; drawing a plug to describe the wrist retinaculum (Image 1) can increase understanding of the pathophysiology of carpal tunnel symptoms and be a simple start from which patients can improve their understanding.
While anecdotal evidence for the benefits of drawing in the consultation is plentiful, research is limited: A team at Edinburgh university were the first to document the use of drawing amongst 100 surgeons, 92% of whom valued drawing in surgical practice2. Similarly, the vast majority of patients valued drawing in moderate or complex surgery consent explanations3. There is plenty of evidence for the neurological and cognitive benefits of using images in undergraduate and postgraduate pedagogy4, alongside the cognitive processing of learning5.

Before I studied medicine I attended the Glasgow School Of Art, reading Visual Communication. I was taught to consider what it was I wanted to say, and then work out how best to communicate it visually. This meant considering which material to use and to capture the spirit of the subject I was drawing using appropriately descriptive markings. This trained me to describe the essence of a concept or object and its function or position in the world. These principles can add value to a consultation as drawing supplements or contextualises the words we use. It can improve a patient’s understanding of physiology, pathology and pharmacology and reduce health anxiety; there is evidence that patient drawings can predict health outcomes and provide doctors with more insight into the patient experience6. Cartoons can be particularly helpful to explain pharmacology, particularly for those with limited literacy (Image 2). Colour is important – the red of an inflamed tympanic membrane, or a different colour to demonstrate a middle ear effusion. Just a few different pens can improve understanding.
My patients often ask to keep the drawings that I do (sometimes with the patient’s help) in a consultation as it represents their understanding of what was said. I see drawing as an adjunct in communication and possibly as a way to reduce complaints that can arise when patients feel that they have not been heard.
The use of images is not one-way as patients may add their own drawing, or bring pictures on their mobile device6. The following drawings (with patient permission) show personal representation of the pain experience in cluster headache (Image 3) and in these descriptive sketches (Image 4) the pain of end stage osteoarthritis with spondylolisthesis. Reference to the feeling of dragging and vice-like pain can be seen. I am not alone – there are other professionals using imagery in medicine.



Professor Gabrielle Finn fosters a network of artists, scientists, educators and health professionals interested in alternative methods of displaying by painting anatomical structures directly onto the body. She has kindly given permission for an image to be used here (Image 5). Her work crosses specialties and encourages innovative alternative approaches to learning.
The team around Professor Paul Rea, Professor of Digital and Anatomical Education at the University of Glasgow, created an animation explaining hypertension using clay models which simply describe concepts which are difficult to describe verbally.
Professor Alice Roberts, Professor of the Public Engagement in Science at the University of Birmingham, uploads anatomical videos of embryological folding, and musculoskeletal anatomy, sometimes with the help of Jelly Babies.
In summary, at times there is a need in the doctor-patient consultation to change or extend the communication style. We can let our patients take over the pen to illustrate their concerns or symptoms. Good communication within the GP consultation and the use of alternative techniques to describe issues are valuable tools : sometime words fall short.
This blog was written by Dr Holly Quinton, GP and Illustrator. All images in this blog were provided by Holly with patients' consent. You can read more about Holly and visual consultations in the following BJGP article: How I use drawing and creative processes within the GP consultation.
References:
1Hall JA, Roter DL, Rand CSJ Health Soc Behav. 1981 Mar; 22(1):18-30
2Keenan I, Hutchinson J, Bell K, 2017, 'Twelve tips for implementing artistic learning approaches in anatomy education', MedEdPublish, 6, [2], 44, https://doi.org/10.15694/mep.2017.000106
3 Duffy FD, Gordon GH, Whelan G, Cole-Kelly K, Frankel R, Buffone N, Lofton S, Wallace M, Goode L, Langdon L; Participants in the American Academy on Physician and Patient's Conference on Education and Evaluation of Competence in Communication and Interpersonal Skills. Assessing competence in communication and interpersonal skills: the Kalamazoo II report. Acad Med. 2004 Jun;79(6):495-507. doi: 10.1097/00001888-200406000-00002. PMID: 15165967.
4 Keenan I, Hutchinson J, Bell K, 2017, 'Twelve tips for implementing artistic learning approaches in anatomy education', MedEdPublish, 6, [2], 44, https://doi.org/10.15694/mep.2017.000106
5 C Kotei: Metaphors in Medicine Synapsis Journal Oct 2017
6 Daeboudt, Broadbent, Berger & Kaptein, Lupus, 20,290-289