Royal College of General Practitioners - Online Learning Environment
Site blog
Written by Dr Toni Hazell
Menopause and hormone replacement therapy (HRT) has become a hot topic in the last few years, with celebrity endorsement for various treatments (some evidence based, others not so much!) and a greater understanding of the multiple ways in which the menopause and perimenopause can present. As well as hot flushes and night sweats (vasomotor symptoms/VMS), symptoms can include insomnia, reduction in energy levels, cognitive dysfunction or ‘brain fog’, low mood, headaches and genitourinary symptoms1.
Many women will benefit from the use of HRT, but it is unsuitable for some (for example due to a history of breast cancer), and others prefer not to use it. Alternative options may be bought over the counter or prescribed and as of March 2026 there is one more non-HRT possibility available on the NHS, with the NICE approval of fezolinetant.
Women who would rather use a herbal option will find plenty to choose from on their local high street or online - isoflavones, soya products, black cohosh, St. John’s wort and red clover are all marketed to treat the menopause. There is some evidence for black cohosh (though use is often limited by adverse effects including constipation and weight gain); there are only poor-quality studies available for other herbal options. Many herbal options have natural oestrogenic activity, and the British Menopause Society (BMS) therefore cautions against their use in women who have had breast cancer. This is not the case for St. John’s wort, which is mentioned in the NICE guidance on menopause as something that may relieve VMS in women who have had breast cancer3. As an enzyme inducer, it does however have many interactions with other drugs that we prescribe, including some such as warfarin for which change in drug levels can have serious implications. Most herbal preparations are not regulated in the same way as prescribed medication, meaning that the amount of active ingredient can vary between products. Women who wish to use herbal treatments for their menopause could be usefully signposted to information from the Women’s Health Concern4 and advised to look for preparations which carry the Traditional Herbal Registration (THR) mark5. This indicates that the product has been registered with the Medicines and Healthcare Regulatory Agency (MHRA) and meets MHRA standards for quality and safety. A list of preparations with a THR mark is available on the MHRA website6 and includes several products used for symptoms of the menopause.
Menopause-specific cognitive behavioural therapy (CBT) is another hormone-free option, although access on the NHS may vary. It can be delivered face to face or remotely and to an individual or in group sessions3 and has evidence for reduction in VMS severity, stress and insomnia, as well as being particularly useful for those women who have diagnosed anxiety or depression related to their menopause.
Prescribable options include selective serotonin re-uptake inhibitors (SSRIs), serotonin–norepinephrine reuptake inhibitors (SNRIs), clonidine, drugs which affect the gamma-amino butyric acid (GABA) receptors, fezolinetant and oxybutynin. More information on these is given in the table below2,3,7,8. We should also remember that all women (whether or not they take HRT) can benefit from lifestyle advice in the (peri)menopause – weight-bearing exercise will reduce osteoporosis risk, exercise in general can improve mood and there is some evidence for the benefits of a Mediterranean diet to improve VMS9.
|
|
Evidence base |
NICE |
Other points |
|
SSRI SNRI |
|
|
|
|
Clonidine |
|
|
|
|
Oxybutynin |
|
|
|
|
GABA drugs |
|
|
|
|
Fezolinetant |
|
|
|
RCGP eLearning Feedback
We greatly value your commitment to lifelong learning and to maintaining the highest standards of patient care. Your feedback plays a crucial role in helping us improve the CPD products and services we offer. Please could you complete our short RCGP eLearning feedback form, which will take no more than 5 minutes as your insights will directly inform the development of future learning experiences that are relevant, practical, and tailored to your needs as a GP.
References:
- BMS. What is the menopause? January 2026. [Accessed May 2026].
- BMS. Non-hormonal-based treatments for menopausal symptoms. November 2025. [Accessed May 2026].
- NICE. NG23. Menopause: identification and management. April 2026. [Accessed May 2026].
- WHC. Complementary and alternative therapies. November 2025. [Accessed May 2026].
- MHRA. The Traditional Herbal Registration (THR) Certification Mark: Guidance for Business. [Accessed May 2026].
- MHRA. Herbal medicines granted a traditional herbal registration (THR). October 2025. [Accessed May 2026].
- NICE. TA1143. Fezolinetant for treating moderate to severe vasomotor symptoms associated with menopause. March 2026. [Accessed May 2026].
- MHRA. Fezolinetant▼(Veoza): risk of liver injury; new recommendations to minimise risk. April 2025. [Accessed May 2026].
- Kennard A, Lindo FM, Ring M et al. Lifestyle Medicine and Vasomotor Symptoms: An Analytic Review. Am J Lifestyle Med. 2024 Feb 27:15598276241232359.
Written by Dr Dirk Pilat
Tuberculosis (TB) is an infectious disease caused by one of the bacteria in the Mycobacterium tuberculosis (Mtb) complex. It is spread by droplets containing the bacteria released by patients with active TB when they speak, cough or sing. Depending on the environment, the droplets can stay in air for hours1. It is currently not clear how many people completely clear an initial infection with Mtb, but it is believed that up to 20% of people who come in contact with TB do not become infected (so called resisters)2. Of those not resisting infection, the vast majority develop latent TB, but a small subset of patients will develop active disease. Patients with latent TB host a small number of live but inactive TB bacteria, are asymptomatic and cannot spread the infection to others. Nevertheless, 5-10% will develop active TB in their lifetimes3. According to the World Health Organization (WHO) up to one third of the world’s population is estimated to be infected with M. tuberculosis, and the vast majority have no signs or symptoms of TB disease, although they are at risk for active TB disease and for becoming infectious at a later stage4.
The highest incidence of active TB is in the first year after infection and decreases thereafter, with young children most at risk. In people with active lung disease, the most common presentation is a cough, although systemic symptoms such as fever or weight loss are common. In children, the only symptoms of tuberculosis might be poor weight gain and lethargy.
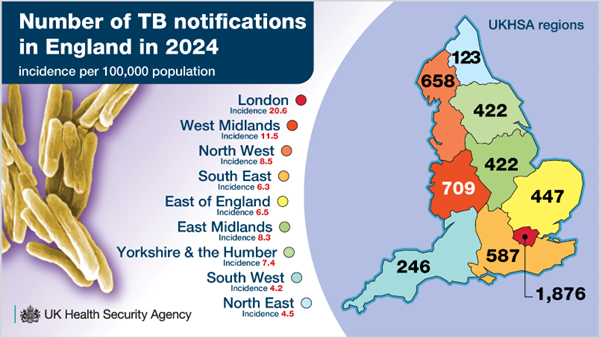
Figure 1 UKHSA TB infographics 2025
In 2026 the United Kingdom’s Health Security Agency (UKHSA) reported the steepest annual increase in tuberculosis cases in England (5490) since national surveillance began, which gives the UK some of the highest TB rates in Western Europe. Wales reported 95 cases in 2024, Scotland 266 and Northern Ireland 865,6,7 . While incidence remains the highest in densely populated areas such, rates are rising in the West Midlands, (22.7%), Yorkshire and the Humber (19.2%) and the Southwest (17.7%). The WHO noted that there was a small increase of people falling ill with TB compared to the previous notification period (2022) worldwide, with 87% of notifications coming from 30 high burden TB countries.
81.9% of TB notifications are for people born outside the UK, with the highest proportion from India, followed by Pakistan, Nigeria and Romania. More than 50% of notified individuals had pulmonary TB. Almost a quarter of patients had had least one co-morbidity such as diabetes, immunosuppression or chronic kidney disease (CKD).
People from high incidence countries who want to stay more than six weeks in the UK need to undergo pre-entry screening with a chest x-ray: of 700 000 checked through this route, just under 400 people were diagnosed with pulmonary TB8,9 .
For those diagnosed here in the UK, the UKHSA reports a link between social deprivation and TB, with current or previous homelessness the most common social risk factor (SRF).
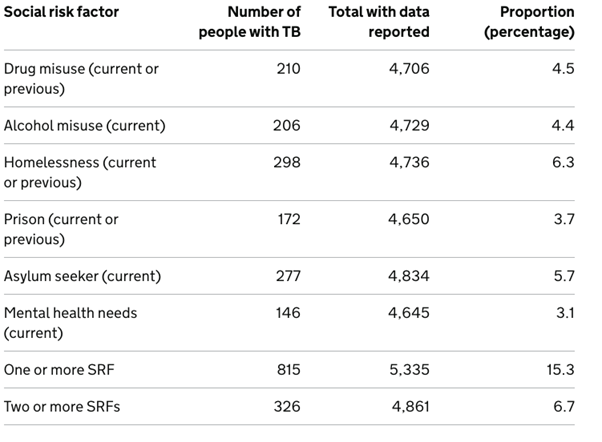
Table 1 Proportions of people aged 15 or more with individual social risk factors (SRFs), England 2024. UKHSA 2026
To improve pick up rates in the community, the ICBs with the highest TB Burden in England have a testing and treatment programme for latent infection that aims to test 25% of new entrants in the UK who arrived within the last five years. NICE believes that primary care has a role to play as well, by suggesting that primary care staff should arrange testing for all vulnerable migrants not previously checked (although this is not part of core funding)10.
For patients who present acutely in primary care, consider a diagnosis of active TB for those with cough, fever, night sweats, weight loss, or fatigue in settings with a high incidence of disease, or in patients without symptoms who have epidemiological risk factors such as HIV, particularly from countries with a high incidence11.
Pathways for referral may vary from locality to locality, but a call to the local TB service will help to avoid confusion and decide whether a referral is urgent or routine. Some services request that general practice initiates investigations such as chest x-ray, three sets of sputum for acid-fast bacillus (AFB) and TB culture and one sputum for routine culture12.
For those patients with suspected TB involving the central nervous system, TB neurological symptoms or those who are systemically unwell, consider urgent admission.
While TB as a disease is mostly managed by our colleagues in secondary care, we can nevertheless contribute to a lowering of the local infection rate by being vigilant and having a low referral threshold.
RCGP eLearning Feedback
We greatly value your commitment to lifelong learning and to maintaining the highest standards of patient care. Your feedback plays a crucial role in helping us improve the CPD products and services we offer. Please could you complete our short RCGP eLearning feedback form, which will take no more than 5 minutes as your insights will directly inform the development of future learning experiences that are relevant, practical, and tailored to your needs as a GP.
References:
- Centre for disease control and prevention (CDC). Tuberculosis: Causes and How It Spreads. 2025. [Accessed March 2026].
- de Martino M, Lodi L, Galli L and Chiappini E. Immune Response to Mycobacterium tuberculosis: A Narrative Review. 2019. Frontiers in Pediatrics. 7:350. doi: 10.3389/fped.2019.00350
- CDC. Clinical Overview of Latent Tuberculosis Infection. 2024. [Accessed April 2026].
- World Health Organization. Latent tuberculosis infection; Updated and consolidated guidelines for programmatic management. 2018. [Accessed March 2026].
- Public Health Wales. Tuberculosis in Wales Annual Report 2024. 2025. [Accessed March 2026].
- Public Health Scotland. Tuberculosis annual report for Scotland 2024. 2025. [Accessed March 2026].
- Public Health Agency NI. TB still on the increase in Northern Ireland. 2025. [Accessed March 2026].
- UKHSA. Tuberculosis prevention, England, 2024. 2026. [Accessed March 2026].
- UKHSA. Tuberculosis incidence and epidemiology, England. 2024. [Accessed March 2026].
- NICE NG33. Tuberculosis. 2024. [Accessed March 2026].
- Nathavitharana R R, Jijon D F, Pal P, Rane S. Diagnosing active tuberculosis in primary care. 2021. BMJ. 374 :n1590 doi:10.1136/bmj.n1590
- Sidhu, Misha. Referrals to ESNEFT (Colchester site) Tuberculosis service. 2025. [Accessed March 2026].
Written by Dr Toni Hazell
In an increasingly anti-vaccination world, it should be gratifying to see the phones of clinics and pharmacies ringing off the hook as parents try to get their teenagers vaccinated against meningitis B, but vaccines are best delivered in an orderly fashion rather than due to parental panic. What is going on here? Why do we suddenly have an outbreak of meningitis B, what is being done to control it, and what needs to happen in the longer term?
Meningococcal disease is caused by Neisseria meningitidis, a Gram-negative diplococcus which occurs in 12 capsular groups – A, B, C, E, H, I, K, L, W, X, Y and Z. Of these, B, C, W and Y are most likely to cause invasive disease in the UK; this usually presents with meningitis or septicaemia, although it can also affect other organ systems, causing pneumonia, myocarditis and endocarditis among other clinical presentations. Meningococcal disease has a high fatality rate (5-10%) and is most common in infants under the age of one, with a secondary peak at age 15 – 19. Survivors may face complications which include limb loss, seizures and loss of vision or hearing1.
NHS vaccination against meningitis B (2 doses) is offered as part of the newborn vaccination programme, with a booster at one year. Vaccination against strains A, C, W and Y is given in schools at the age of 142. Vaccination has resulted in a significant drop in the incidence of invasive meningococcal disease in the UK, but the meningitis B vaccination programme only started in 20152, so children over the age of 10 remain unprotected by the NHS. An adolescent meningitis B vaccination programme was considered by the Joint Committee on Vaccination and Immunisation in 2013, but rejected on the grounds of cost-effectiveness, because there wasn’t strong evidence that vaccination protected against meningococcal disease3. Charities are now calling for all adolescents to be vaccinated using a booster programme4.
This unprotected cohort includes those starting university, a time where young people will bring together different strains of infectious diseases from around the country, traditionally leading to ‘freshers flu’. Occasionally this mingling of unvaccinated people from different geographic areas has more tragic consequences, as has happened recently in Kent, where there are currently (as of 01.04.26) 21 confirmed cases of meningococcal disease and two fatalities, all with an epidemiological link to a particular nightclub5.
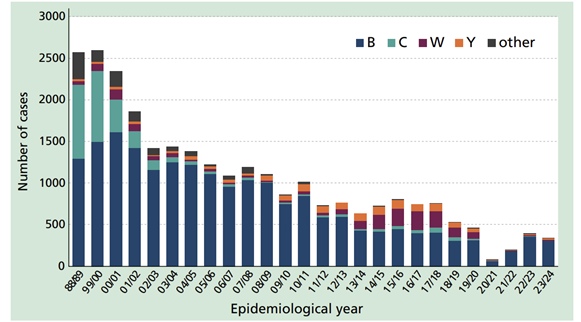
Cases of invasive meningococcal disease by epidemiological year, England and Wales 1998-2021. Public sector content available under the Open Government Licence v3.01
GPs may be affected by this outbreak in a variety of ways. They might receive requests for vaccination against meningitis B, might see patients presenting for antibiotic prophylaxis, or may have an increased number of patients presenting because they think that they have meningitis, being more aware of possible symptoms due to the press coverage. The latter request would be dealt with in the same way as any presentation of acute illness and a request for vaccination should be dealt with as usual – there is currently no national programme offering NHS vaccination outside of the usual regimen, with the only extra vaccinations being those targeted at students in Kent. Those who missed their adolescent dose of the Men ACWY vaccine can be offered it on the NHS up to their 25th birthday1, whereas those who missed their newborn dose of the MenB vaccine can only have it up to their second birthday. At the time of writing, most private pharmacies and clinics have run out of vaccine and are adding those who request it to a waiting list.
Regarding prophylaxis, clinics have been set up locally to the university to offer prophylactic antibiotics to the following groups7:
- All students who live on Canterbury campus.
- All staff who live or work in affected halls of residence.
- Anyone who attended Club Chemistry on 5, 6 and 7 March.
- Close contacts who have been identified by UKHSA.
NHSE have asked that GPs provide this prophylaxis, an unlicensed one-off dose of ciprofloxacin (as per the table below) where students have already travelled home and so cannot collect it from the clinics in Kent7. Contractually, the provision of antibiotic prophylaxis in an outbreak is the job of public health rather than the GP; some areas manage this by contracting this work to certain sites (such as an out of hours centre) or funding the GP to do it via an enhanced service or memorandum of understanding. Check what the system is in your area if you’re not sure.
Ciprofloxacin prophylaxis dose6

This is an evolving event, and it remains to be seen what longer-lasting effects this outbreak has, in terms of the behaviour of the public in accessing private vaccinations and decisions on NHS meningitis B vaccination for the missed cohort.
References
- UKHSA. Meningococcal: the green book, chapter 22. July 2025.
- NHS. NHS vaccinations and when to have them. Aug 2023.
- UK Parliament. Meningitis: Vaccination. Question for Department of Health and Social Care. Dec 2025.
- Meningitis now. No Plan B for MenB.
- UKHSA. Cases of invasive meningococcal disease notified in Kent. March 2026.
- NHS. MenB vaccine for children. March 2024.
- NHSE. Outbreak of meningococcal disease linked to University of Kent and the area of Canterbury. March 2026
Written by Dr Dirk Pilat
The NHS Bowel Cancer screening programme was first rolled out across the United Kingdom in 2006, using the guaiac faecal occult bood test (gFOBT). It was initially only offered to people between 60 and 70, but subsequently extended to 74 (patients over 75 can request tests if they would like to continue testing1). gFOBT was replaced from 2017 to 2021 across the NHS with the faecal immunochemical test (FIT) and extended to younger people2. The stool guaiac test had various issues: a long list of medications could potentially cause false positives, as could certain foods3. It was also trickier to use, as patients had to apply six dollops of faeces from three different bowel motions to a little paper envelope, reducing the acceptability of the test4. The FIT testing kit reduced this complexity and added improved acceptability to just a simple scrape of a testing stick across one faecal sample before adding it to a sample bottle5. As FIT uses antibodies to detect the presence of human blood, it is both more sensitive and specific than gFOBT6.

Figure 1 FIT sample container. By Whispyhistory - Own work, CC BY-SA 4.0,
The move to FIT caused an increase of screening uptake from under 60% to nearly 70%. Since the introduction of bowel cancer screening in England, the incidence of colorectal cancer in adults fell by 7%. For 2023 to 2024, NHS England:
- Invited 6,969,227 people to take part in screening
- 4,710,330 of them took up the offer of screening, an overall uptake of 67.6%
- 83,112 (1.76%) of the people screened were invited back for further tests
- screening led to 35,039 colonoscopies where at least one high risk polyp was detected
- 5,320 bowel cancers were found – a detection rate of 0.11%7.
Across England, Scotland and Wales, eligibility for bowel cancer screening starts at 50 and ends at 74, with biannual invitations. In Northern Ireland eligibility is from 60 to 748.
While the current FIT threshold for referral in England and Northern Ireland is 120 μg Hb/g, Wales has already lowered its threshold for referral to 80μg Hb/g and Scotland has always set its FIT threshold at 80μg Hb/g. In symptomatic patients who had their FIT arranged in primary care, NICE suggests to refer using a suspected cancer pathway referral for colorectal cancer if they have a FIT result of at least 10 micrograms of haemoglobin per gram of faeces9.
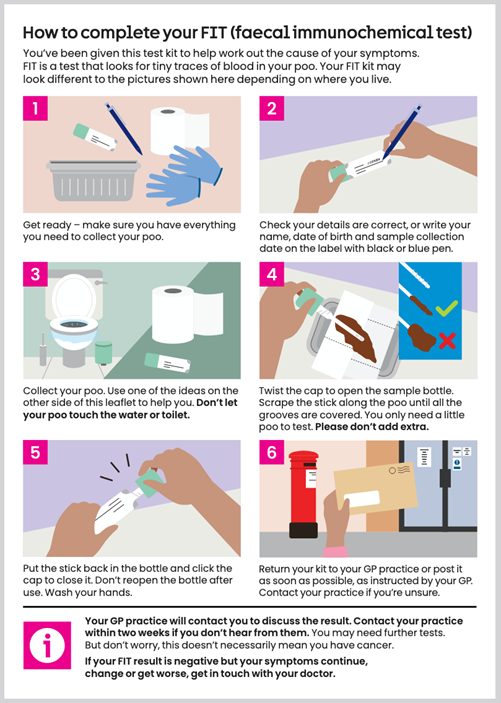
Figure 2 FIT instructions by Cancer Research UK
In 2026 the threshold in England is being lowered to 80μg Hb/g in a phased rollout that should be completed by March 2028. This will likely increase the amount of positive screening results by 36%, resulting in the detection of an extra 2017 high risk polyps and 663 more bowel cancers.
While bowel screening is not part of day to day general practice, we still have an important role to play: encouraging to take part in the screening activity by their general practitioner results in a significant increase in uptake10 and the use of our computerised patient management systems can help here, as we are being notified if patients are not participating.
We know that more than half of patients having to undergo a colonoscopy experience anxiety around the procedure. This is due to worries about bowel preparation, difficulties with the procedure (embarrassment, pain, possible complications, and sedation), and concerns about the diagnosis - including fear of being diagnosed with cancer11. With the increase in recalls, our patients’ concerns are likely going to lead to an increased amount of people contacting their primary care teams, fearful of going ahead with the examination. We can signpost our patients to a detailed (and reassuring) explanation of what happens on the day of their colonoscopy provided by the NHS.
Reassurance from their primary care team can go a long way to allay a patient’s concerns and support them in partaking in this important screening programme.
References
- NHS. Bowel Cancer Screening. 2024.
- Whyte S, Sun Y. T. ModelHealth and Resource Consequences of Reducing the Faecal Immunochemical Test(FIT) Screening Threshold for Colonoscopy in the NHS Bowel Cancer Screening Programme (BCSP) [accessed February 2026].
- Kaur K, Zubair M, Adamski JJ. Fecal Occult Blood Test. December 2025 [accessed February 2026].
- Strachan H. Wealth of evidence highlights the benefits of bowel cancer screening UK National Screening Committee 2025. [accessed February 2026].
- Cancer research UK. How to collect your FIT. [accessed February 2026].
- Alpha Laboratories. About Faecal Immunochemical Testing - What is a FIT?[accessed February 2026].
- Strachan H. Wealth of evidence highlights the benefits of bowel cancer screening UK National Screening Committee 2025. [accessed February 2026].
- Bowel Cancer UK. Bowel cancer screening | About bowel cancer. 2019. [accessed February 2026].
- NICE. Suspected cancer: recognition and referral. 2026. [accessed February 2026].
- Triantafillidis JK, Vagianos C, Gikas A, et al. Screening for colorectal cancer:the role of the primary care physician. European Journal of Gastroenterology & Hepatology. 2017 Jan 1; 29(1): e1–7. [accessed February 2026].
-
Yang C, Sriranjan V, Abou-Setta AM, et al. Anxiety Associated with Colonoscopy and Flexible Sigmoidoscopy: A Systematic Review. American Journal of Gastroenterology. 2018 Dec; 113 (12): 1810–8.
Written by Dr Toni Hazell
It wasn’t what I wanted in my stocking as a child, but as a full-blown contraception nerd, I’m excited at the December 2025 launch of the new UK Medical Eligibility Criteria for contraceptive use (UKMEC)1. Published by the College of Sexual and Reproductive Healthcare (CoSRH), formerly the Faculty of Sexual and Reproductive Healthcare, the UKMEC is the gold-standard document on contraceptive safety.
Before getting into the changes, there are some important basics to remember:
- The UKMEC is about safety, not efficacy, although the document does include an efficacy table (figure 1).
- Methods are categorised from 1-4, as per figure 2. 1 and 4 are simple – no problem to use or absolutely contraindicated respectively; it’s in the 2s and 3s that your clinical judgment will be important.
- The UKMEC is one place where 2 + 2 ≠ 4. Two category 2s doesn’t automatically mean an absolute contraindication, but if they are both in the same area, it does signal a cumulative risk and the need for caution. More than one category 3 ‘may pose an unacceptable risk’.1
- Some methods have different numbers for initiation or continuation, reflecting the different risks attached to starting a method or continuing one that is already being used.
- If a condition isn’t covered in the UKMEC, that doesn’t necessarily mean that all contraception is safe for use. Consider seeking advice from secondary care, or, if you are a CoSRH member, submit an evidence request to their Clinical Effectiveness Unit and they will summarise the available evidence for you to use alongside your clinical judgment.2
- The UKMEC is intended to be applied only to contraceptive use. If a woman is getting an extra benefit from her method (for example the management of endometriosis), that may affect your risk/benefit calculation.
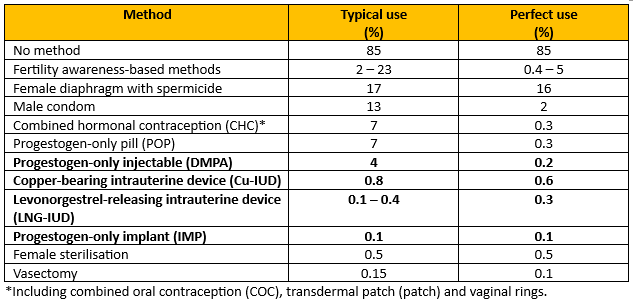
Figure 1 - Recreation of Percentage of women experiencing an unintended pregnancy within the first year of year of use with typical use and perfect use.
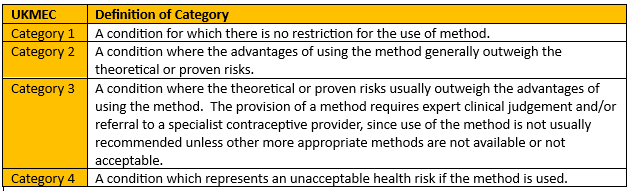
Figure 2 - Recreation of Definition of UKMEC categories
The key changes are summarised in figure 3.
|
Topic(s) |
Key change |
|
Chronic kidney disease. Multiple sclerosis.
|
|
|
Use of e-cigarettes. Sickle cell trait. |
|
|
Multiple category changes for the depot medroxyprogesterone acetate (DMPA) injection. |
|
|
Depression and anxiety |
|
|
Stroke |
|
|
Breast cancer |
|
|
Human papilloma virus and sexually transmitted infections. |
|
|
HIV |
|
|
Hypertension |
|
|
Multiple risk factors for VTE and CVD |
|
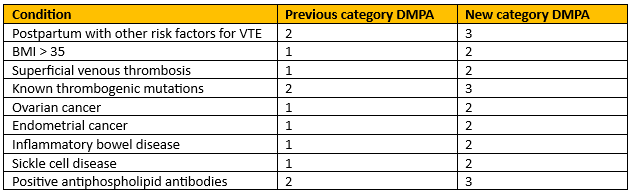
Figure 4 - Recreation of Conditions with increased risk of thrombosis.
Chronic Kidney Disease
Regarding CKD, only the most seriously affected are included – patients who either have nephrotic syndrome or are on dialysis. This cohort should not use CHC (due to VTE risk), and DMPA is now UKMEC 3. This is because DMPA is associated with a small loss in bone mineral density, reversible on stopping3 and those with chronic kidney disease (CKD) are already at risk of osteoporosis4. All other methods are a UKMEC 2.
Multiple sclerosis
The risk from MS is mainly to do with immobility as a risk factor for VTE, so most methods are a UKMEC 1 for those without prolonged immobility, the exception being DMPA, which is a 2, because those with MS have a greater risk of fracture than the greater population. With prolonged immobility, DMPA remains a 2 and CHC is a 3.
When prescribing hormonal contraception, it is common to be asked about whether it will cause mood changes. Mood alteration is listed as a common or very common side-effect in the BNF for some combined and progestogen only methods5,6,7 but depression was listed in the previous UKMEC as a category 1. It has been removed from this edition as a category and replaced with a statement about the effects of hormonal contraception in those with anxiety or mood disorders.
The key points are as follows8:
- There is no clear evidence that any form of hormonal contraception worsens or improves mood.
- Most evidence is from observational studies, which often have confounding factors, and do not usually focus on women with pre-existing mental health conditions.
- Some patients do report mood change during the use of hormonal contraception; this may not represent direct causation.
- Healthcare professionals should explore other possible contributing factors and consider alternative contraception if the patient feels that their mood has been adversely affected by their contraception.
- Patients with pre-existing anxiety or depression should monitor their mood when starting hormonal contraception.
There are two sections on multiple risk factors – one for CVD and one for VTE; the section on multiple risk factors for VTE has been updated in this iteration. The UKMEC signposts to NICE for a full list of risk factors but gives examples which include cancer, inflammatory disorders, recent trauma or surgery and being in the postnatal period. Someone with multiple risk factors for VTE is UKMEC 4 for CHC, 3 for DMPA and 1 for all other methods.
The UKMEC is a long document; it will take time for the changes to fully bed in, but practices will need to decide how they implement it, particularly for those already using contraception. Reviewing all those using DMPA at the time of their next injection, and everyone else at their annual review would be a good start and hopefully we will all be fully up to date with it long before the next one comes along in a decade or so!
References
- CoSRH. UK Medical Eligibility Criteria for Contraceptive Use (UKMEC). Dec 2025.
- CoSRH. Members’ Evidence Request Service.
- CoSRH. Progestogen-only Injectable Contraception. July 2023.
- National Osteoporosis Guideline Group UK. Clinical guideline for the prevention and treatment of osteoporosis. 2024.
- BNF. Ethinylestradiol with levonorgestrel.2025.
- BNF. Desogestrel.2025.
- BNF. Etonogestrel. 2025.
Written by Dr Toni Hazell
Chickenpox is a common and unpleasant childhood illness. More than 90% of the population have acquired antibodies to the causative infection (the varicella zoster virus) by the age of 151. For many it is a self-limiting illness (often leaving behind scars when scratching cannot be resisted), but there is a risk of significant complications, as listed in the box below. Those at a higher risk of complications include adults, adolescents, children aged under one, pregnant women and immunocompromised people. Around 20 people per year die of chickenpox in the UK3 and there is a risk of neonatal death if a susceptible woman contracts chickenpox in the week before delivery3.
|
Complications of chickenpox1: |
|
The economic cost to the UK of parents taking time off work to provide childcare to their children with chickenpox is estimated to be over £24 million per year4 – the difficulties of taking prolonged time off work for childcare perhaps explains why one survey (the satisfyingly named SPOTTY study5 showed that 73% of UK paediatricians surveyed had privately vaccinated their child against varicella. As the author of this blog discovered last year, chickenpox can also wreak havoc if it appears two days before a family holiday!
Until recently, NHS chickenpox vaccination has only been offered to a small group of people. These include susceptible healthcare staff (including non-clinical, e.g. cleaners, porters etc), laboratory staff who work with the varicella virus, and close household contacts of immunocompromised patients, such as siblings of a child with leukaemia, or a child whose parent is having chemotherapy3. For patients who are due to start immunocompromising medication and are susceptible to varicella, vaccination is offered if there is enough time to give the two-dose course before the medication has to be started3.
This will change in January 2026, when universal vaccination begins on the NHS in all four countries of the UK 6,7,8,9. Details of the programme are as follows10
- Offered to children at the age of 18 months.
- Given with measles, mumps and rubella as the MMRV vaccine.
- Booster at three years and four months of age.
- One-dose catch-up programme for children born between 1.1.2020 and 31.8.22, who can access the vaccine until the end of March 2028.
- No NHS offer of a single varicella vaccine.
- The MMR vaccine without varicella will no longer be available for the NHS routine childhood immunisation programme, although it will still be available for those who need the MMR vaccine in adulthood. Children who did not have MMR at the usual time and are brought later in childhood should be caught up with MMRV.
So why have the Joint Committee on Vaccination and Immunisation (JCVI), who decided against universal childhood varicella vaccination in 2009, changed their mind? The original decision was made on cost-effectiveness grounds, with an estimate that it would take 80-100 years for the programme to become cost-effective11. The new decision has largely been based on two factors – a review of the prevalence of chickenpox complications, and a change in the way we think about shingles in adults.
The JCVI believe that the cost of chickenpox complications has probably been underestimated, affecting their assessment of of cost-effectiveness of the vaccine. It is likely that many people admitted with complications of chickenpox have had their admission coded with the name of the complication (pneumonia, meningitis, cellulitis etc) but that the code for chickenpox was not added, so the two weren’t linked for the purposes of cost calculation11. The availability of the four-virus MMRV vaccine has also improved the cost-effectiveness calculation, as there is no need for another nurse appointment, over and above the one which would have been necessary for the MMR vaccine.
Another concern in 2009 was that vaccinating against chickenpox would put older adults at an increased risk of shingles, caused by reactivation of the varicella virus. The theory was that those who have had chickenpox in the past have their immunity regularly boosted by coming into contact with children who have varicella (which is infectious during the prodrome, before spots have appeared and children are kept at home) and that reducing chickenpox incidence in children would increase shingles in middle-aged adults. At the 2023 review it was clear that data from the United States (who have vaccinated against chickenpox since 1995) did not support this hypothesis11 – and we also now have the NHS shingles vaccination, which was not offered in 2009.
Vaccine hesitancy remains an issue in the UK, with only 85% of English 5 year olds having had two doses of MMR – uptake in some communities is significantly lower than that12. It will be interesting to see whether the addition of varicella to the MMR vaccine reduces uptake further, due to unwarranted nerves about multiple vaccine, or whether the benefits of not having to look after an irritable child with chickenpox will encourage people to vaccinate, in turn increasing MMR uptake.
References
- NICE CKS. Chickenpox. Nov 2023.
- Oxford Vaccine Group. Chickenpox (varicella). Nov 2023.
- UKHSA. Varicella: the green book, chapter 34. Sept 2024.
- LSE. The true cost of chickenpox: at least £24 million in lost productivity a year in the UK. April 2022.
- O'Mahony E, Sherman SM, Marlow R et al. UK paediatricians' attitudes towards the chicken pox vaccine: The SPOTTY study. Vaccine. 2024 Sep 17; 42 (22): 126199.
- DHSC. Free chickenpox vaccination offered for first time to children. Aug 2025.
- Department of health. Chickenpox vaccination to be offered to children in Northern Ireland from 2026. Aug 2025.
- NHS Scotland. Changes to the Scottish Childhood Vaccination Schedule from 1 January 2026 (phase 2) – introduction of a routine Varicella Zoster (Chickenpox) vaccine. Nov 2025.
- NHS Wales. New Chickenpox (Varicella) Vaccination Programme in Wales.
- UKHSA and NHSE. Introduction of a routine varicella (MMRV) vaccination programme for children at one year and at 18 months. Oct 2025.
- DHSC. JCVI statement on a childhood varicella (chickenpox) vaccination programme. Nov 2023.
- UKHSA. Evaluating the impact of national and regional measles catch-up activity on MMR vaccine coverage in England, 2023 to 2024.Aug 2024.
Written by Dr Dirk Pilat
Introduction
Venous thromboembolism (VTE) - whether it presents as deep vein thrombosis (DVT) or pulmonary embolism (PE) - is a common presentation in primary care: its annual incidence is 1-2 cases per 1000 population, rising significantly with increased age. In Europe, pulmonary embolism accounts for 8–13 deaths per 1000 women and 2–7 deaths per 1000 men aged 15–55 years1. Thrombosis UK suggests that 1 in 20 people will experience a VTE in their lifetime2. NHS Resolution reports that from 1 April 2012 until 31 March 2022 it documented 687 closed claims relating to VTE injuries across the clinical negligence indemnity schemes, with total damages paid of £23,780,1793.
Significant risk factors such as major surgery, prolonged immobilisation, and major trauma account for approximately 20% of all venous thromboembolism episodes, though the commonest strong persistent risk factor is active cancer, accounting for approximately 20% of incidents. Table 1 lists persistent and transient risk factors for VTE.
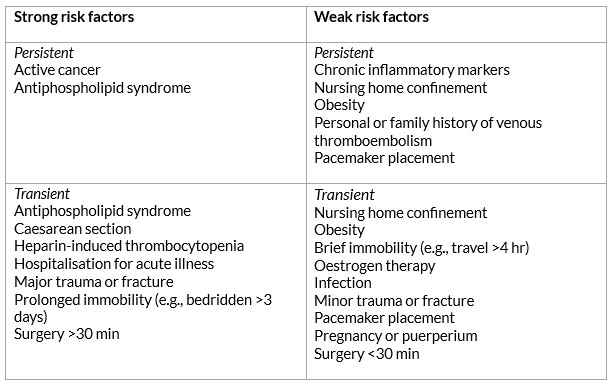
Table 1: Khan F, Tritschler T, Kahn SR, Rodger MA. Venous thromboembolism. The Lancet 2021 Jul; 398(10294): 64–77.
Signs and symptoms
Patients with a deep vein thrombosis can present with leg pain (80–90% of patients), swelling (80%), localised tenderness on palpation (75–85%), prominent collateral superficial veins (30%) and redness (25%). 30% - 60% of patients presenting with a proximal (above the knee) DVT already have a silent pulmonary embolism. A review paper from Canada described that the majority of symptomatic episodes of lower extremity DVTs start in the distal veins, with symptoms being uncommon until there is involvement of the proximal veins. They reported that in a consecutive series of 189 outpatients with a first episode of venographically diagnosed DVT, where symptoms were all distal, 89% had proximal thrombi4. Upper extremity deep vein thrombosis (UEDVT) – arising in the brachial, axillary or subclavian veins - is thought to account for about 10% of all DVTs5.
Pulmonary emboli often present insidiously and often without the classic triad of pleuritic chest pain, shortness of breath and hypoxia. There are a large number of case reports showing patients complaining of nagging symptoms for weeks before succumbing to pulmonary embolism, with 40% of these patients being seen by a physician in the weeks prior to their death6. A retrospective cohort study from 2016 showed that 25% of patients with a PE presenting in primary care had an average delay of 15.7 days to diagnosis7. Table 2 lists the range of symptoms that the NICE CKS suggests point towards a PE.
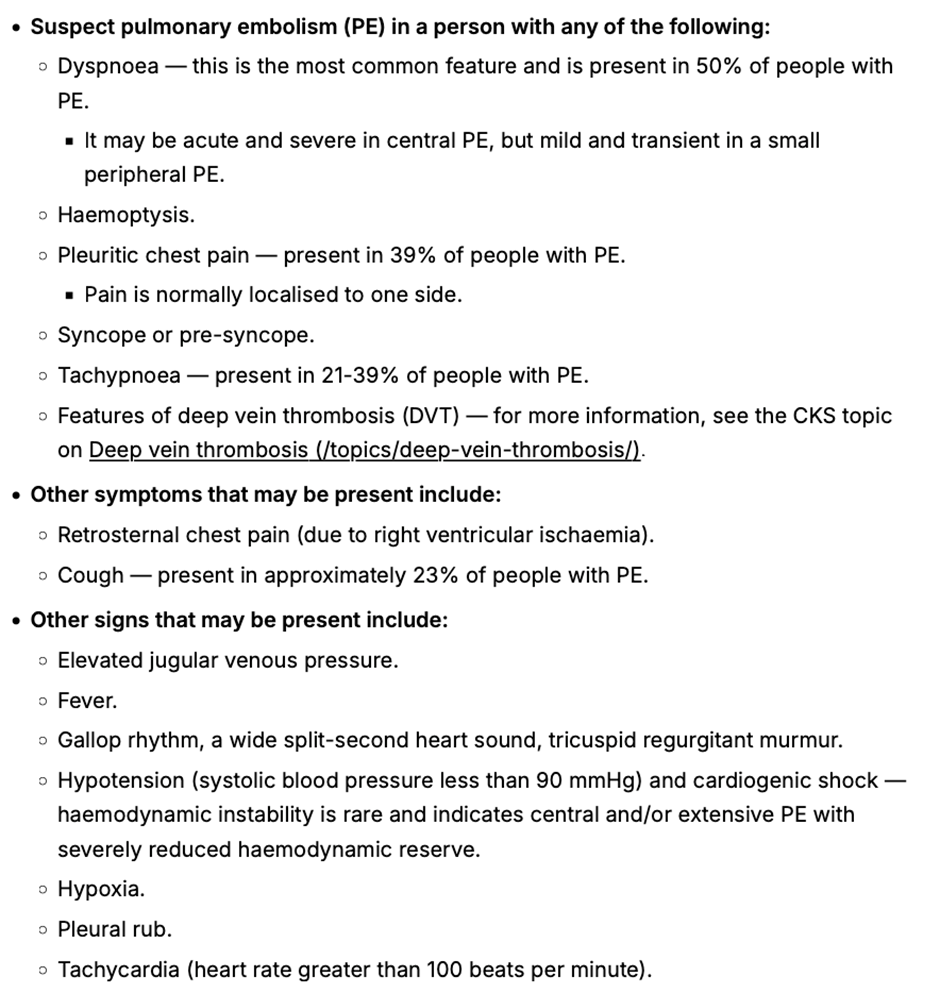
Table 2: When to suspect pulmonary embolism from NICE CKS Pulmonary embolism 2023.
Diagnosis
The National Institute for Health and Care Excellence (NICE) updated their recommendations for the diagnosis and management of VTE in 2023. It suggests that patients with symptoms that might indicate a DVT should be examined and accessed via a 2 - level Wells Score. If the Wells score is 2 or above, these patients should be offered a proximal leg vein ultrasound scan, with the result available within 4 hours if possible. If the scan is negative, a D-Dimer should be arranged. For those patients that can’t access a proximal leg vein ultrasound scan within 4 hours, offer a D‑dimer test, then interim therapeutic anticoagulation and a proximal leg vein ultrasound scan with the result available within 24 hours. For those patients with a Wells score of 1 or less, arrange a D dimer test with the result available within 4 hours, or, if the D dimer test result cannot be obtained within 4 hours, offer interim therapeutic anticoagulation while awaiting the result. If the D-Dimer test is positive, arrange an ultrasound and add interim anticoagulation if not already started (see Table 5)
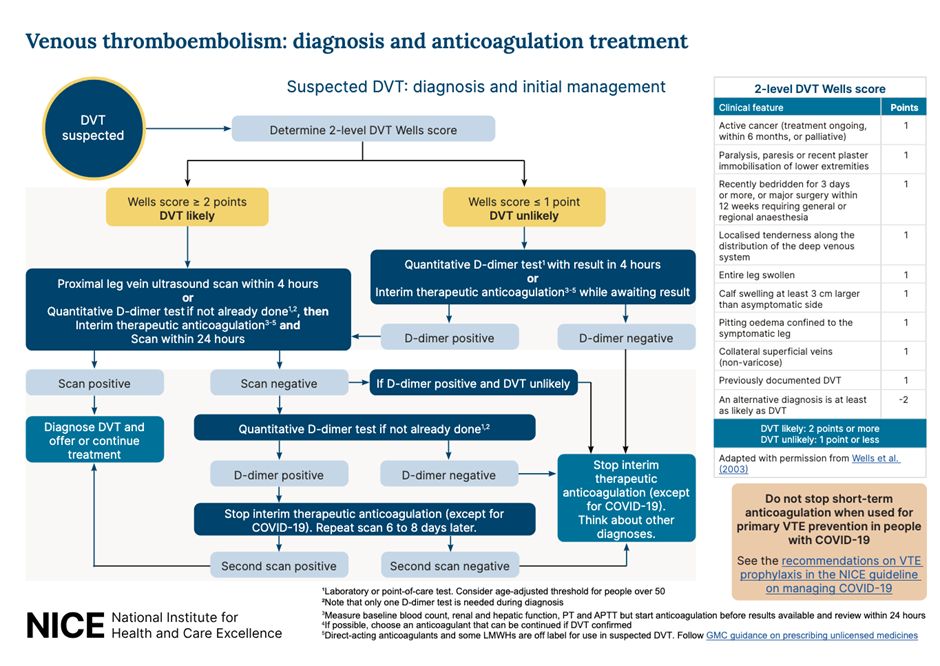
Table 3: Recommended workflow for suspected DVT. NICE 2023
For people who present with signs or symptoms of a PE, arrange a physical examination, take a medical history and offer a chest x-ray (if available in your setting) to exclude other causes. If, after assessment and investigations, the clinical suspicion for a PE is low and other diagnoses are more likely, consider using the pulmonary embolism rule–out criteria to help determine whether any further investigations into a PE are necessary. This questionnaire has not been validated for people with COVID-19.
If a PE is suspected, the 2 level PE Wells score (see table 6) should be used.
If a patient scores 4 or more, NICE suggests a range of different imaging options arranged in secondary care, with anticoagulation to be initiated depending on the outcomes.
If the Wells score is 4 or less, NICE suggests D-Dimer testing with the result being available within 4 hours, or interim anticoagulation if this can’t be arranged. If the D-Dimer is positive, imaging will have to be arranged8
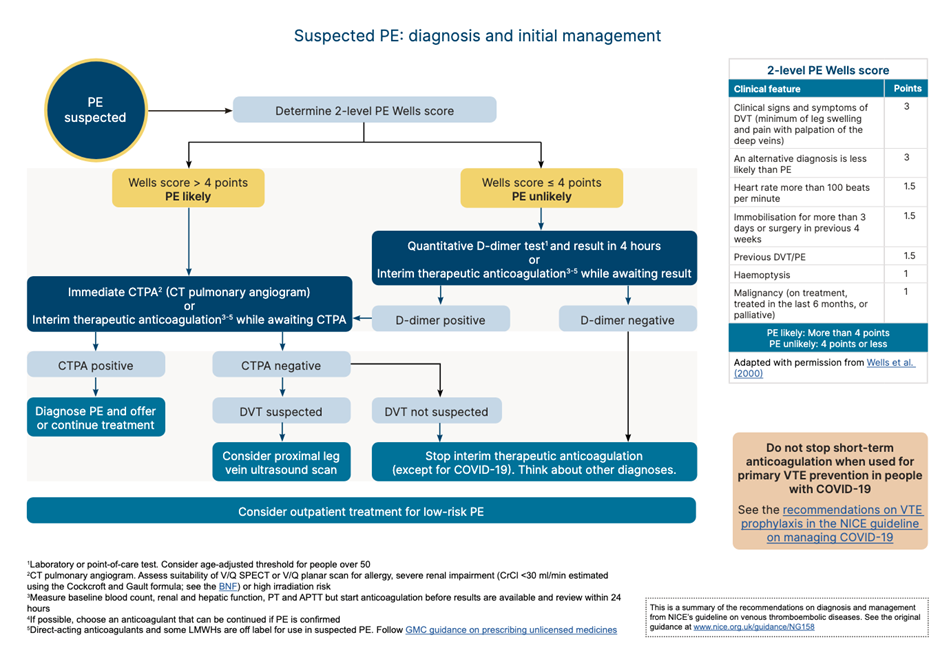
Table 4: Recommended workflow for PE. NICE 2023
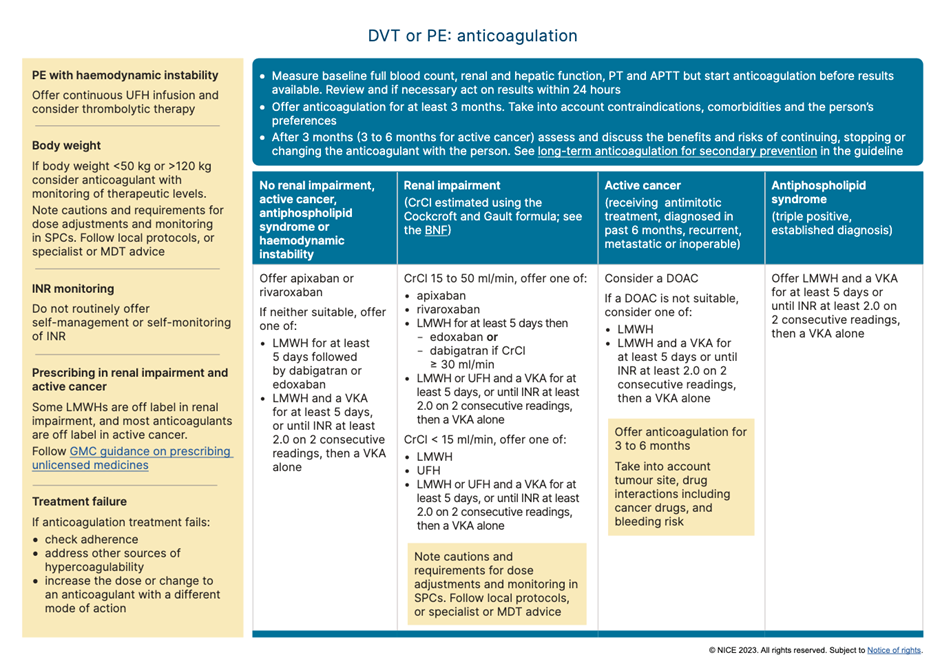
Table 5: Recommendations for anticoagulation for suspected/confirmed VTE. NICE 2023
In day-to-day practice every locality will have their own protocols and referral pathways for the management of suspected VTE in the community. Nevertheless it is important to remember that patients who score 1 or below on the DVT Wells questionnaire, should still have a D-Dimer test. This was highlighted by a case that a coroner shared with the RCGP, in which a patient tragically died four weeks after an initial assessment for calf swelling; while the Wells score was applied, the patient did not have a D-Dimer. The patient then developed respiratory symptoms and was seen by various healthcare practitioners over a 4 week period before suffering a cardiac arrest caused by a large PE.
The vast majority of patients with VTEs are being expertly managed in cooperation between primary and secondary care. General practitioners are experts in managing diagnostic uncertainty - an inevitable part of their profession - and VTE presentations can certainly can test this vital skill. Acknowledging the broad scope of symptoms and subsequent use of the local pathways for VTE can nevertheless increase the pickup rate further, improving the safety of our patients.
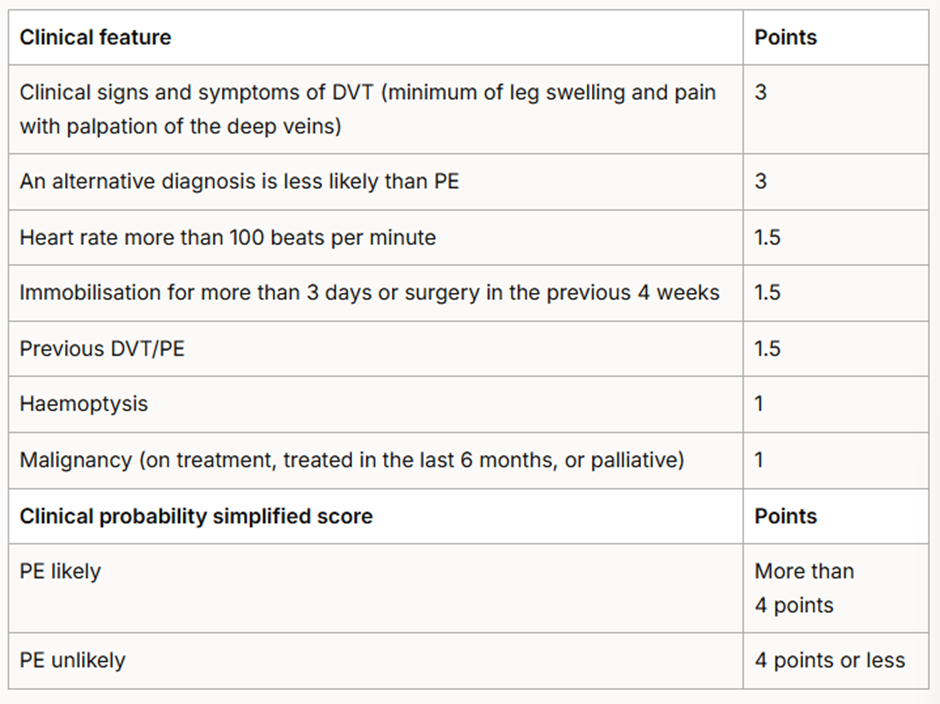
Table 6: Two-level PE Wells score. NICE 2023 Venous thromboembolic diseases: diagnosis, management and thrombophilia testing.
References
- Khan F, Tritschler T, Kahn SR, et al. Venous thromboembolism. The Lancet . 2021 Jul; 398 (10294): 64–77.
- Thrombosis UK.
- Venous thromboembolism. NHS Resolution. 2023.
- Kearon C. Natural History of Venous Thromboembolism. Circulation. 2003 Jun 17; 107 (90231): 22I-30.
- Ageno W, Haas S, Weitz JI, et al. Upper Extremity DVT versus Lower Extremity DVT: Perspectives from the GARFIELD-VTE Registry. Thrombosis and Haemostasis. 2019 Jun 10; 119 (08): 1365–72
- Safi M, Tajik Rostami R, Taherkhani M. Unusual presentation of a massive pulmonary embolism. J Teh Univ Heart Ctr 2011; 6( 1): 41-44.
- Walen S, Damoiseaux RA, Uil SM, et al. Diagnostic delay of pulmonary embolism in primary and secondary care: a retrospective cohort study. British Journal of General Practice. 2016 Apr 25; 66 (647): e444–50.
- National Institute for Health and Care Excellence. NG158 Venous thromboembolic diseases: diagnosis, management and thrombophilia testing 2023.
Written by Dr Toni Hazell
Pneumonia is defined as an infection of the lung tissue, in which the alveoli become filled with micro-organisms, fluid and inflammatory cells, affecting the function of the lungs1. Community acquired pneumonia (CAP) has a mortality rate of around 1% in those who are managed in primary care, rising to up to 14% for those admitted to hospital and to 30% for those who need intensive care1. GPs need to risk stratify and make logical decisions as to who can be managed in the community, and who needs referral and consideration of admission.
An experienced GP will be used to assessing severity of acute infection. We make a clinical assessment, starting with an overall look at the patient (do they look unwell or otherwise make our antennae twitch?), assessment of vital signs such as pulse, respiratory rate, temperature and oxygen saturations, and consideration of co-morbidities such as immunosuppression. The NICE guidance on pneumonia2, published in September 2025, recommends the more formal CRB65 tool, once we have made a clinical diagnosis of pneumonia.
Technology is available to measure C-reactive protein (CRP) as a point of care test in primary care, to help support or refute a diagnosis of inflammation, as occurs in an infection such as pneumonia. A 2016 NICE MedTech innovation briefing3 noted that primary care CRP testing can reduce antibiotic prescribing and referrals for chest x-ray, but that the sensitivity did not rise above 55% (and could be as low as 20% depending on the threshold used). Specificity was better, ranging from 73 – 99%. In the nine years since that briefing, the test has not become widely available, with barriers including cost, lack of commissioning enthusiasm and concern about the evidence base for effectiveness and value for money. A 2025 qualitative review4 comparing the UK with Sweden, the Netherlands and Canada, found that uptake of primary care CRP testing was higher in the other countries, but that clinicians didn’t feel that it had made a huge improvement to their assessment of patients with possible pneumonia, with some saying that the introduction was a policy failure, and the test over-used. Other studies have shown that CRP use is associated with increased antibiotic prescribing, rather than helping to reassure that antibiotics aren’t needed, and that this is particularly associated with systems where a CRP is checked before the patient is seen, resulting potentially in spurious high results in those with a low pre-test probability of bacterial infection5. NICE does not discuss primary care CRP in its latest guideline2, but where it is being used the Primary Care Respiratory Society suggests cut-offs of 20 and 40 mg/L – do not prescribe antibiotics with CRP<20, consider prescribing with CRP of 20-40 if there is purulent sputum, and prescribe with CRP>406.
The CRB65 scoring system is outlined in the box below and the results predict the risk of death in the next 30 days. Zero is low risk (<1%), 1 or 2 intermediate risk (1 – 10%) and 3 or 4 high risk (>10%).
CRB65 score – one point for each of the following:
- Confusion (new disorientation in person, place or time, or a score of ≤8 on an abbreviated mental test).
- Respiratory rate ≥30.
- Blood pressure ≤60 mmHg diastolic or 90 mmHg systolic.
- Age ≥65.
NICE write ‘guidelines not tramlines’7, and this guideline acknowledges the holistic nature of our assessment, advising the use of clinical judgment along with the CRB65 score, which can be affected by other factors such as comorbidities or pregnancy. NICE advises considering referral with a CRB65 score ≥2, and that those with a CRB65 score of 1 might benefit from an assessment in a same-day emergency care unit (which is in any case often where those referred to hospital will end up) or by being referred to a virtual ward or hospital at home service. Those with a score of zero can be managed in primary care, with appropriate safety-netting to return if symptoms deteriorate. Any signs of significant complications, such as heart failure, would lower the threshold for referral. We should have a lower threshold for children and young people (those aged under 18), considering referral or specialist advice for every patient.
For those not admitted, we would usually treat pneumonia with antibiotics in the community, to be started as soon as possible after the clinical diagnosis has been made2. Whilst some causes are viral, the majority of pneumonia has a bacterial cause1, and we cannot reliably differentiate between the two. The commonest bacterial cause is Streptococcus pneumoniae, with other responsible organisms including Haemophilus influenzae, Staphylococcus aureus and the atypical Mycoplasma pneumoniae. Those who are immunocompromised, or who have had multiple recent courses of antibiotics, may be more likely to have an unusual or drug-resistant bacteria (or a fungal infection such as Aspergillus) as a cause for their pneumonia8,9; pneumonia in those with an unsafe swallow may be related to aspiration of stomach contents10.
NICE emphasises the need for only a five day course of antibiotics for adults and three days for children aged up to 11, with a longer duration only when clinically necessary. This may be because they have had a temperature in the last 48 hours of the five day course, or that they continue to have a sign of clinical instability, such as (in adults) systolic blood pressure <90 mmHg, heart rate >100 bpm, respiratory rate >24 breaths per minute or oxygen saturations <90% on air. These parameters, if present after five days of antibiotics, might make us re-visit the decision to keep the patient at home. The suggested first-line antibiotic for low-severity disease is amoxicillin, with doxycycline or clarithromycin as second-line, and erythromycin for pregnant women. For moderate severity disease the choice is largely the same, although clarithromycin moves to first line if an atypical bacterial cause is suspected. Those with high-severity disease are likely to be in hospital, but if treated in the community then a combination of co-amoxiclav and clarithromycin are first line, with erythromycin in pregnancy and levofloxacin as an alternative for those with penicillin allergy (bearing in mind the MHRA advice on quinolones11).
Distinguishing between typical and atypical bacterial causes without a sputum sample is by no means an exact science; those with an atypical bacteria may have more prolonged or prominent constitutional symptoms (headache, malaise, sore throat, fever) and may be less likely to have clear consolidation on auscultation of the chest. Atypical infection can come in epidemics, with many cases clustered together and then none for several years and is more common with increasing age and in those who live in enclosed spaces such as boarding schools or military barracks. Outbreaks of one particular atypical bacteria, Legionella pneumophila are associated with contaminated water and air-conditioning systems and another, Legionalla longbeachae is associated with exposure to contaminated soil mixtures12. Consideration of an atypical bacteria should be given when the patient doesn’t respond to an apparently appropriate first-line choice of antibiotic, and where there is a history of staying in a hotel or resort where exposure may be more likely.
Further reading and useful resources
- RCGP eLearning modules on Aspergillus and pneumonia.
- NICE guidance on pneumonia.
- StatPearls articles on aspiration pneumonia, atypical pneumonia and pneumonia in the immunocompromised patient.
- Patient information leaflet and NHS webpage on pneumonia.
References
- NICE CKS. Chest infections – adult. Jan 2025.
- NICE. NG250. Pneumonia: diagnosis and management. Sept 2025.
- NICE. MIB81. Alere Afinion CRP for C-reactive protein testing in primary care. Sept 2016.
- Glover RE, Pacho A, Mays N. C-reactive protein diagnostic test uptake in primary care: a qualitative study of the UK's 2019-2024 AMR National Action Plan and lessons learnt from Sweden, the Netherlands and British Columbia. BMJ Open. 2025 Aug 31;15(8):e095059.
- Payne R, Mills S, Wilkinson C et al. Point-of-care C-reactive protein testing in general practice out-of-hours services: tool or trap? Br J Gen Pract. 2025 Aug 28;75(758):388-389.
- Primary Care Respiratory Society. The place of point of care testing for C-reactive protein in the community care of respiratory tract infections. Summer 2022.
- Reeve J. Avoiding harm: Tackling problematic polypharmacy through strengthening expert generalist practice. Br J Clin Pharmacol. 2021 Jan;87(1):76-83.
- Aleem MS, Sexton R, Akella J. Pneumonia in an Immunocompromised Patient. [Updated 2023 Jul 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025.
- Assefa M. Multi-drug resistant gram-negative bacterial pneumonia: etiology, risk factors, and drug resistance patterns. Pneumonia (Nathan). 2022 May 5;14(1):4.
- Sanivarapu RR, Vaqar S, Gibson J. Aspiration Pneumonia. [Updated 2024 Mar 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-.
- MHRA. Fluoroquinolone antibiotics: must now only be prescribed when other commonly recommended antibiotics are inappropriate. Jan 2024.
- Nguyen AD, Stamm DR, Stankewicz HA. Atypical Bacterial Pneumonia. [Updated 2025 Apr 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-.
Written by Dr Emma Nash
The Chief Medical Officer’s low-risk drinking guidelines recommend that adults do not drink more than 14 units of alcohol a week, spread evenly over three or more days.1
Although around 20% of the population report drinking no alcohol at all, a significant proportion of adults regularly drink over the recommended amount, ranging from 9% of Northern Irish women to 32% of English men.2 The consequences of excessive alcohol consumption are significant, with 10,473 deaths from alcohol-specific causes in the UK in 20233; many more are alcohol-related.
The public health approach ‘Making Every Contact Count’ (MECC)4 promotes the importance of making the most of opportunities to effect behaviour change. It encourages the use of routine interactions with people to offer brief advice and support them in making positive changes to their physical and mental health and wellbeing. Alcohol brief interventions are one such example.
In the context of alcohol, a brief intervention can be described as: “a short, evidence-based, structured conversation about alcohol consumption with a patient that seeks in a non-confrontational way to motivate and support the individual to think about and/or plan a change in their drinking behaviour in order to reduce their consumption and/or their risk of harm”.5
Brief interventions take 5-15 minutes to deliver and are ideally reinforced over further sessions. Multiple models exist, but ultimately the purpose is to focus the person’s attention on their lifestyle, highlight the reasons for change and potential strategies to do it, and empower the person to make the change. Whilst time constraints make a GP consultation challenging to deliver this, even a very brief intervention, with follow-up to discuss further, is useful.
Enquiring is the first stage – simple questions about alcohol consumption, or something more structured such as an AUDIT-C – can help identify where there is a problem, or at least bring it to mind. Behavioural change is a process rather than an event and even moving from the pre-contemplation to the contemplation stage of change is positive.
The brief intervention itself varies in form and needs specific training dependent on the model used. However, a common theme is motivational interviewing. Key elements of motivational interviewing include an emphasis on patient autonomy and patient-centred collaborative approach built on acceptance. One model of motivational interviewing by Miller and Rollnick6 describes four processes:
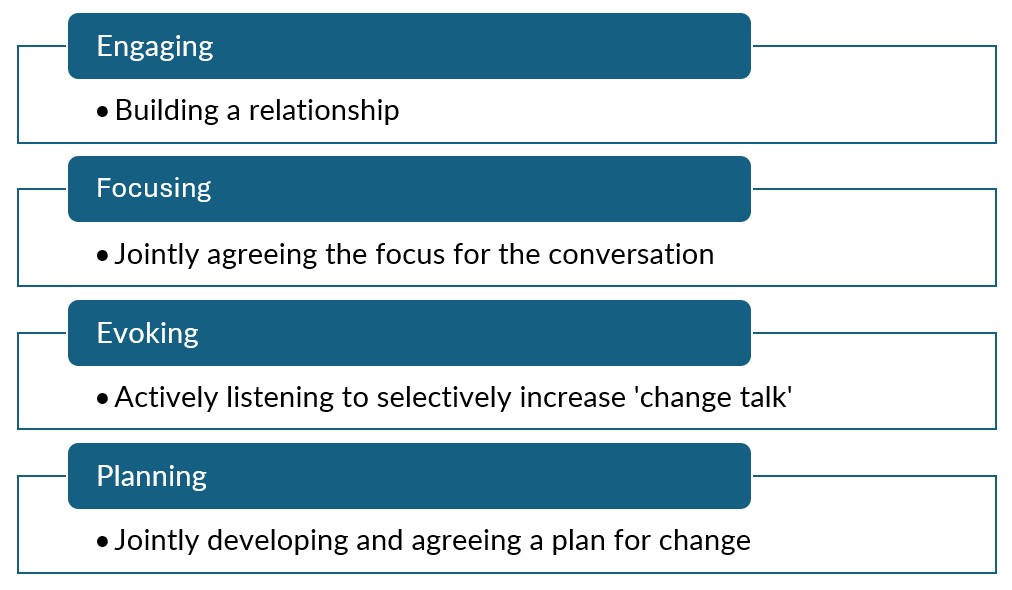
The extent to which motivational interviewing features in the brief intervention depends on the particular model chosen.7
One example of a brief intervention tool is the FRAMES model.8,9
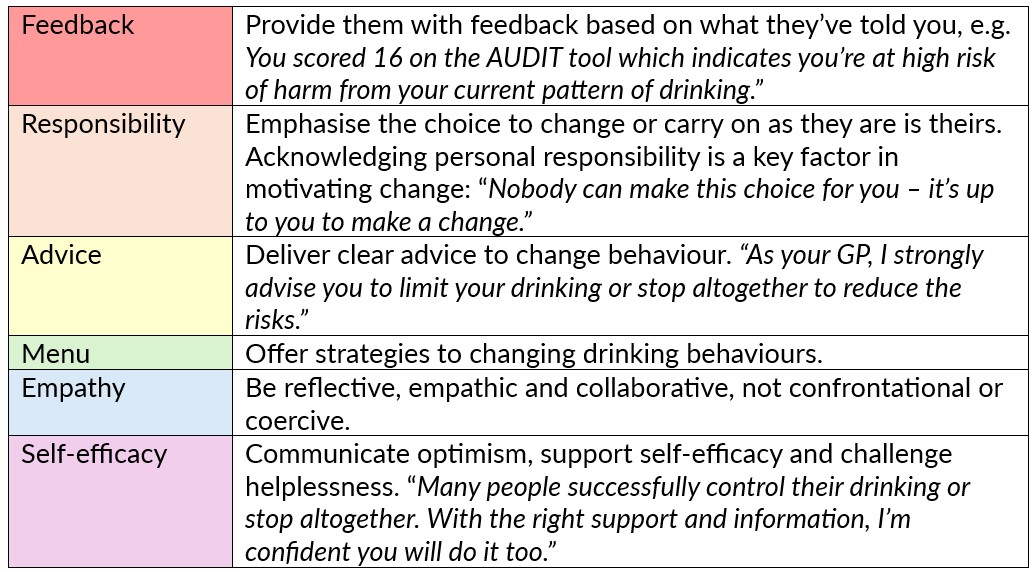
What you are able to suggest in the ‘Menu’ section depends on what is available locally in terms of support. However, behavioural strategies may include setting personal drinking limits and sticking to it; alternating alcoholic drinks with soft drinks; switching to low alcohol drinks; having regular alcohol-free days; identifying high risk situations for heavy drinking and creating a management plan; engaging in alternative activities to drinking.
Whilst these interventions can appear complex or arduous, they are only brief and are designed to be delivered in snippets, with reinforcement. The evidence base for the use of brief interventions is good, particularly in a primary care setting10,11 and have the potential to have a significant impact on the future health of our patients.
Further reading
National Institute on Alcohol Abuse and Alcoholism. Conduct a brief intervention: Build motivation and a plan for change.
NHS England. eLFH - Alcohol identification and brief advice.
ScotPHO. Alcohol: treatment for alcohol misuse.
References
- English, Scottish, Welsh and Northern Irish Governments. UK Chief Medical Officers’ Low Risk Drinking Guidelines. 2016.
- Alcohol Change UK. Alcohol statistics. Updated 2025.
- Office for National Statistics. Alcohol-specific deaths in the UK: registered in 2023. 2025.
- Public Health England, NHS England, Health Education England. Making Every Contact Count (MECC): Consensus statement. 2016.
- Scottish Government. Local delivery plan: Alcohol brief interventions. National guidance 2019-2020. 2019.
- Miller WR, Rollnick S. Motivational Interviewing, 3rd ed. Helping people change. New York (NY): Guilford Press; 2012.
- World Health Organisation. Alcohol brief intervention training manual for primary care. WHO, 2017.
- Bien T, Miller WR, Tonigan JS. Brief interventions for alcohol problems: a review. Addiction, 1993. 88(3): p.315-336.
- Drug and Alcohol Clinical Advisory Service. Fact sheet. FRAMES – Brief intervention for risky or harmful alcohol consumption.
- World Health Organisation. Global status report on alcohol and health 2014. Luxembourg: WHO, 2014.
- Platt L, Melendez-Torres GJ, O'Donnell A, et al How effective are brief interventions in reducing alcohol consumption: do the setting, practitioner group and content matter? Findings from a systematic review and metaregression analysis. BMJ Open 2016; 6: e011473.
Written by Dr Dirk Pilat
There is no question that general practice is an increasingly stressful profession, with ever growing demands placed on GPs while battling with diminishing financial and staffing resources. Days at work that just won’t end, never-ending workload and little control over our working lives can affect even the most resilient of practitioners. Throw in the constant battle with complaints and medicolegal issues and it’s no wonder that the prevalence of burnout, depression, low self-esteem and anxiety are significantly higher in the medical profession compared with the general population1. The numbers are startling: An MDDUS survey from 2024 reported 71% of general practitioners suffering from compassion fatigue and 65% suffering from burnout2. A PULSE survey from 2025 found that more than 54% of primary care doctors had to reduce sessions due to stress3. Unfortunately doctors aren’t great patients: we tend to downplay the severity of our symptoms and under-diagnose conditions in ourselves and often ignore the fact that we should seek help4.
For some time now, but particularly during and after the COVID-19 pandemic, attempts have been made to prevent burnout syndrome through individual and systemic approaches within the primary care workforce. Various psychological interventions were developed to empower professionals coping with increasing stress and burnout. Mindfulness-based interventions (MBI) are effective in reducing stress and promoting self-care and wellbeing: there is a growing body of research evidence that these can increase job satisfaction and even improve patient outcomes. Mindfulness has a well-established evidence base showing efficacy in improving the psychological wellbeing in both clinical and non-clinical populations. Various MBIs exist, though mindfulness-based stress reduction (MBSR) is the most extensively reviewed. Originally designed for patients with chronic medical and psychological conditions, it improves quality of life via focussed attention exercises, cognitive restructuring and adaptive learning techniques5. A 2020 systematic review of mindfulness – based stress reduction interventions on the psychological functioning of healthcare professionals showed that this particular method reduced anxiety, depression and stress and increased self-compassion6.
A 2021 systematic review on the impact of psychological Interventions with elements of mindfulness for physicians came to a similar conclusion: the vast majority of studies showed a positive impact on empathy, well-being, and reduction of burnout7. Similarly, a 2016 mixed method study showed that general practitioners who learned mindfulness based stress reduction (MBSR) techniques as a part of their regular CPD programme showed a significant decrease in depersonalisation and an increase in dedication and mindfulness skills compared with the control group8.
Interestingly, a decline in empathy and an increase in stress levels is not only experienced by established general practitioners but also by medical students and young doctors during their training. At the Charité – the medical faculty of the Freie Universität Berlin and Humboldt-Universität zu Berlin - medical students can choose to take part in a voluntary course on stress reduction. Delivered over one semester, students are being taught methods of mindfulness and meditation with quantitative results showing a reduction in perceived stress and an increase in self-efficacy, mindfulness, self-reflection and empathy9, confirming previous results of similar interventions, including previously obtained long-term results of this course format showing effects on stress biomarkers10.
For those struggling to find the time to engage in MBI, the ubiquitousness of wearable technological devices such as smart watches and mobile phones can – rather counter-intuitively – help to take part in short activities helping to achieve emotional control in the middle of a busy day. An example for this is the ‘Mindfulness app’ on the Apple Watch (similar apps exist on Android-based devices). A small 2024 mixed method study invited participants to engage for 5 minutes daily with the application, trying to achieve 6 breaths per minute during usage. After two weeks the data showed this to result in a significant increase in participants’ coping skills and slight reduction in symptoms of depression and anxiety11.
In these stressful days it feels important to identify strategies to the improve quality of life for the primary care workforce. For some, mindfulness-based interventions might be just the ticket, even when it’s only for 5 minutes a day.
References:
- Society of Occupational Medicine. What could make a difference to the mental health of UK doctors? A review of the research evidence. 2018.
- MDDUS. Compassion fatigue in healthcare professionals 2024.
- Colivicchi A. More than half of GPs reduced their sessions due to work-related stress. Pulse Today. 2025.
- Best, Ho. What’s it like to be a patient as a doctor. British Medical Journal 2024 Oct 11; q1486–6.
- Kabat-Zinn, Jon. Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness. New York: Bantam Books, 2013
- Kriakous SA, Elliott KA, Lamers C, et al. The Effectiveness of mindfulness-based Stress Reduction on the Psychological Functioning of Healthcare professionals: a Systematic Review. Mindfulness. 2021 Sep 24; 12 (1): 1–28.
- Tement S, Ketiš ZK, Miroševič Š, et al. The Impact of Psychological Interventions with Elements of Mindfulness (PIM) on Empathy, Well-Being, and Reduction of Burnout in Physicians: A Systematic Review. International Journal of Environmental Research and Public Health. 2021 Oct 25; 18 (21): 11181.
- Verweij H, Waumans RC, Smeijers D, et al. Mindfulness-based stress reduction for GPs: results of a controlled mixed methods pilot study in Dutch primary care. British Journal of General Practice. 2016 Jan 28; 66 (643): e99–105.
- Brinkhaus B, Stöckigt B, Witt CM, et al. Reducing stress, strengthening resilience and self-care in medical students through Mind-Body Medicine (MBM). 2025 Jan 1; 42 (1): Doc7–7.
- MacLaughlin BW, Wang D, Noone AM, et al. Stress Biomarkers in Medical Students Participating in a Mind Body Medicine Skills Program. Evidence-Based Complementary and Alternative Medicine. 2011; 2011: 1–8.
- Wright SL, Bach E, Bryson SP, et al. Using an App-Based Mindfulness Intervention: A Mixed Methods Approach. Cognitive and behavioral practice. 2024 Apr 1.