_ RCGP Learning
Blog entry by _ RCGP Learning
Written by Dr Toni Hazell
In an increasingly anti-vaccination world, it should be gratifying to see the phones of clinics and pharmacies ringing off the hook as parents try to get their teenagers vaccinated against meningitis B, but vaccines are best delivered in an orderly fashion rather than due to parental panic. What is going on here? Why do we suddenly have an outbreak of meningitis B, what is being done to control it, and what needs to happen in the longer term?
Meningococcal disease is caused by Neisseria meningitidis, a Gram-negative diplococcus which occurs in 12 capsular groups – A, B, C, E, H, I, K, L, W, X, Y and Z. Of these, B, C, W and Y are most likely to cause invasive disease in the UK; this usually presents with meningitis or septicaemia, although it can also affect other organ systems, causing pneumonia, myocarditis and endocarditis among other clinical presentations. Meningococcal disease has a high fatality rate (5-10%) and is most common in infants under the age of one, with a secondary peak at age 15 – 19. Survivors may face complications which include limb loss, seizures and loss of vision or hearing1.
NHS vaccination against meningitis B (2 doses) is offered as part of the newborn vaccination programme, with a booster at one year. Vaccination against strains A, C, W and Y is given in schools at the age of 142. Vaccination has resulted in a significant drop in the incidence of invasive meningococcal disease in the UK, but the meningitis B vaccination programme only started in 20152, so children over the age of 10 remain unprotected by the NHS. An adolescent meningitis B vaccination programme was considered by the Joint Committee on Vaccination and Immunisation in 2013, but rejected on the grounds of cost-effectiveness, because there wasn’t strong evidence that vaccination protected against meningococcal disease3. Charities are now calling for all adolescents to be vaccinated using a booster programme4.
This unprotected cohort includes those starting university, a time where young people will bring together different strains of infectious diseases from around the country, traditionally leading to ‘freshers flu’. Occasionally this mingling of unvaccinated people from different geographic areas has more tragic consequences, as has happened recently in Kent, where there are currently (as of 01.04.26) 21 confirmed cases of meningococcal disease and two fatalities, all with an epidemiological link to a particular nightclub5.
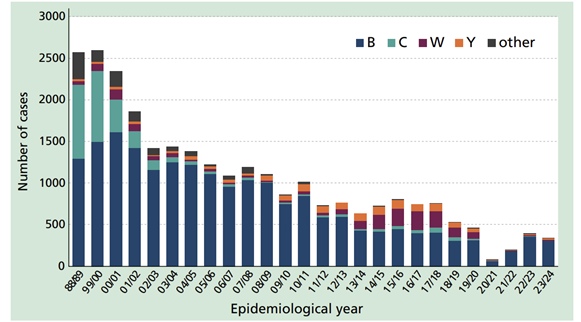
Cases of invasive meningococcal disease by epidemiological year, England and Wales 1998-2021. Public sector content available under the Open Government Licence v3.01
GPs may be affected by this outbreak in a variety of ways. They might receive requests for vaccination against meningitis B, might see patients presenting for antibiotic prophylaxis, or may have an increased number of patients presenting because they think that they have meningitis, being more aware of possible symptoms due to the press coverage. The latter request would be dealt with in the same way as any presentation of acute illness and a request for vaccination should be dealt with as usual – there is currently no national programme offering NHS vaccination outside of the usual regimen, with the only extra vaccinations being those targeted at students in Kent. Those who missed their adolescent dose of the Men ACWY vaccine can be offered it on the NHS up to their 25th birthday1, whereas those who missed their newborn dose of the MenB vaccine can only have it up to their second birthday. At the time of writing, most private pharmacies and clinics have run out of vaccine and are adding those who request it to a waiting list.
Regarding prophylaxis, clinics have been set up locally to the university to offer prophylactic antibiotics to the following groups7:
- All students who live on Canterbury campus.
- All staff who live or work in affected halls of residence.
- Anyone who attended Club Chemistry on 5, 6 and 7 March.
- Close contacts who have been identified by UKHSA.
NHSE have asked that GPs provide this prophylaxis, an unlicensed one-off dose of ciprofloxacin (as per the table below) where students have already travelled home and so cannot collect it from the clinics in Kent7. Contractually, the provision of antibiotic prophylaxis in an outbreak is the job of public health rather than the GP; some areas manage this by contracting this work to certain sites (such as an out of hours centre) or funding the GP to do it via an enhanced service or memorandum of understanding. Check what the system is in your area if you’re not sure.
Ciprofloxacin prophylaxis dose6

This is an evolving event, and it remains to be seen what longer-lasting effects this outbreak has, in terms of the behaviour of the public in accessing private vaccinations and decisions on NHS meningitis B vaccination for the missed cohort.
References
- UKHSA. Meningococcal: the green book, chapter 22. July 2025.
- NHS. NHS vaccinations and when to have them. Aug 2023.
- UK Parliament. Meningitis: Vaccination. Question for Department of Health and Social Care. Dec 2025.
- Meningitis now. No Plan B for MenB.
- UKHSA. Cases of invasive meningococcal disease notified in Kent. March 2026.
- NHS. MenB vaccine for children. March 2024.
- NHSE. Outbreak of meningococcal disease linked to University of Kent and the area of Canterbury. March 2026