_ RCGP Learning
Blog entry by _ RCGP Learning
Written by Dr Dirk Pilat
Tuberculosis (TB) is an infectious disease caused by one of the bacteria in the Mycobacterium tuberculosis (Mtb) complex. It is spread by droplets containing the bacteria released by patients with active TB when they speak, cough or sing. Depending on the environment, the droplets can stay in air for hours1. It is currently not clear how many people completely clear an initial infection with Mtb, but it is believed that up to 20% of people who come in contact with TB do not become infected (so called resisters)2. Of those not resisting infection, the vast majority develop latent TB, but a small subset of patients will develop active disease. Patients with latent TB host a small number of live but inactive TB bacteria, are asymptomatic and cannot spread the infection to others. Nevertheless, 5-10% will develop active TB in their lifetimes3. According to the World Health Organization (WHO) up to one third of the world’s population is estimated to be infected with M. tuberculosis, and the vast majority have no signs or symptoms of TB disease, although they are at risk for active TB disease and for becoming infectious at a later stage4.
The highest incidence of active TB is in the first year after infection and decreases thereafter, with young children most at risk. In people with active lung disease, the most common presentation is a cough, although systemic symptoms such as fever or weight loss are common. In children, the only symptoms of tuberculosis might be poor weight gain and lethargy.
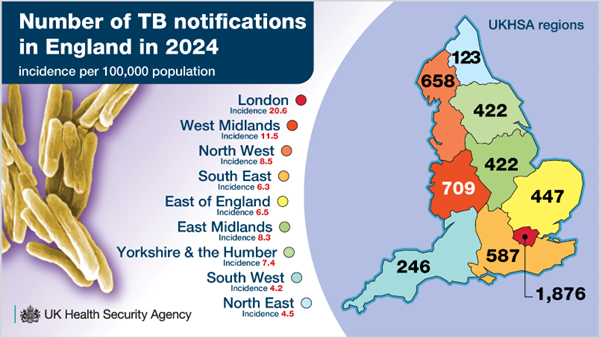
Figure 1 UKHSA TB infographics 2025
In 2026 the United Kingdom’s Health Security Agency (UKHSA) reported the steepest annual increase in tuberculosis cases in England (5490) since national surveillance began, which gives the UK some of the highest TB rates in Western Europe. Wales reported 95 cases in 2024, Scotland 266 and Northern Ireland 865,6,7 . While incidence remains the highest in densely populated areas such, rates are rising in the West Midlands, (22.7%), Yorkshire and the Humber (19.2%) and the Southwest (17.7%). The WHO noted that there was a small increase of people falling ill with TB compared to the previous notification period (2022) worldwide, with 87% of notifications coming from 30 high burden TB countries.
81.9% of TB notifications are for people born outside the UK, with the highest proportion from India, followed by Pakistan, Nigeria and Romania. More than 50% of notified individuals had pulmonary TB. Almost a quarter of patients had had least one co-morbidity such as diabetes, immunosuppression or chronic kidney disease (CKD).
People from high incidence countries who want to stay more than six weeks in the UK need to undergo pre-entry screening with a chest x-ray: of 700 000 checked through this route, just under 400 people were diagnosed with pulmonary TB8,9 .
For those diagnosed here in the UK, the UKHSA reports a link between social deprivation and TB, with current or previous homelessness the most common social risk factor (SRF).
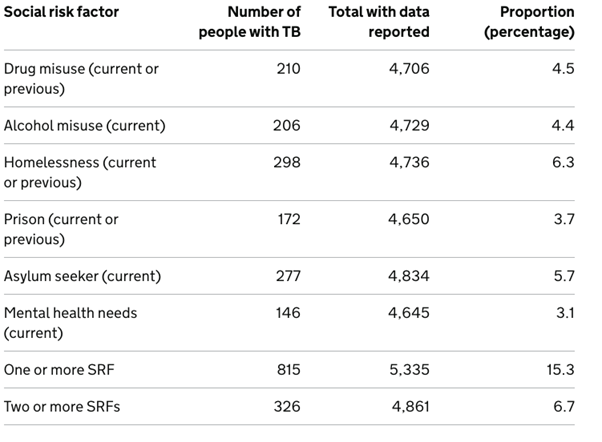
Table 1 Proportions of people aged 15 or more with individual social risk factors (SRFs), England 2024. UKHSA 2026
To improve pick up rates in the community, the ICBs with the highest TB Burden in England have a testing and treatment programme for latent infection that aims to test 25% of new entrants in the UK who arrived within the last five years. NICE believes that primary care has a role to play as well, by suggesting that primary care staff should arrange testing for all vulnerable migrants not previously checked (although this is not part of core funding)10.
For patients who present acutely in primary care, consider a diagnosis of active TB for those with cough, fever, night sweats, weight loss, or fatigue in settings with a high incidence of disease, or in patients without symptoms who have epidemiological risk factors such as HIV, particularly from countries with a high incidence11.
Pathways for referral may vary from locality to locality, but a call to the local TB service will help to avoid confusion and decide whether a referral is urgent or routine. Some services request that general practice initiates investigations such as chest x-ray, three sets of sputum for acid-fast bacillus (AFB) and TB culture and one sputum for routine culture12.
For those patients with suspected TB involving the central nervous system, TB neurological symptoms or those who are systemically unwell, consider urgent admission.
While TB as a disease is mostly managed by our colleagues in secondary care, we can nevertheless contribute to a lowering of the local infection rate by being vigilant and having a low referral threshold.
RCGP eLearning Feedback
We greatly value your commitment to lifelong learning and to maintaining the highest standards of patient care. Your feedback plays a crucial role in helping us improve the CPD products and services we offer. Please could you complete our short RCGP eLearning feedback form, which will take no more than 5 minutes as your insights will directly inform the development of future learning experiences that are relevant, practical, and tailored to your needs as a GP.
References:
- Centre for disease control and prevention (CDC). Tuberculosis: Causes and How It Spreads. 2025. [Accessed March 2026].
- de Martino M, Lodi L, Galli L and Chiappini E. Immune Response to Mycobacterium tuberculosis: A Narrative Review. 2019. Frontiers in Pediatrics. 7:350. doi: 10.3389/fped.2019.00350
- CDC. Clinical Overview of Latent Tuberculosis Infection. 2024. [Accessed April 2026].
- World Health Organization. Latent tuberculosis infection; Updated and consolidated guidelines for programmatic management. 2018. [Accessed March 2026].
- Public Health Wales. Tuberculosis in Wales Annual Report 2024. 2025. [Accessed March 2026].
- Public Health Scotland. Tuberculosis annual report for Scotland 2024. 2025. [Accessed March 2026].
- Public Health Agency NI. TB still on the increase in Northern Ireland. 2025. [Accessed March 2026].
- UKHSA. Tuberculosis prevention, England, 2024. 2026. [Accessed March 2026].
- UKHSA. Tuberculosis incidence and epidemiology, England. 2024. [Accessed March 2026].
- NICE NG33. Tuberculosis. 2024. [Accessed March 2026].
- Nathavitharana R R, Jijon D F, Pal P, Rane S. Diagnosing active tuberculosis in primary care. 2021. BMJ. 374 :n1590 doi:10.1136/bmj.n1590
- Sidhu, Misha. Referrals to ESNEFT (Colchester site) Tuberculosis service. 2025. [Accessed March 2026].